

















Introduction
Mitral valve disease represents an important health problem worldwide [1, 2]. During the last few months a series of articles were published on this topic in the E-Journal of Cardiology Practice [3-26] in addition to the 2017 Guidelines from the ESC/EACTS [27] and ACC/AHA on the management of valvular heart disease [28], as well as a large number of original papers. The aim of the current review is to highlight what could be the key points for our practice.
Mitral regurgitation
Mitral regurgitation (MR) is the first most frequent left-sided valve disease in the community and the second in patients hospitalised [1]. It is now acknowledged that two entities should be separated: primary (organic) MR where the disease of the valve is the cause, and secondary (functional) where the valve is normal and MR is the consequence of dysfunction of the surrounding structures. Primary MR is largely dominated by degenerative disease. Secondary MR is a heterogeneous entity where the leading cause is left ventricular (LV) dysfunction, mostly of ischaemic origin. The importance of annular dilatation related to supraventricular arrhythmias and/or left atrial (LA) dilatation was recently emphasised. Goliasch et al have recently shown that secondary MR is an independent prognostic variable in specific subgroups of patients with an “intermediate-HF severity-phenotype”. Among patients with more advanced HF, myocardial dysfunction is largely dominant and MR seems no longer to have a prognostic impact [29]. This supports an early management in such cases.
Evaluation
The first step in the evaluation of MR should be clinical examination looking for symptoms, abnormal auscultation, and the presence of comorbidity. A recent survey conducted by the ESC in 500 primary care physicians (PCP) and cardiologists from seven countries using case scenarios showed that auscultation is performed by PCPs in only 54% of asymptomatic patients [30].
Echocardiography
Echocardiography, in the majority of cases transthoracic examination (transthoracic echocardiography [TTE]), is the best method for diagnosing MR and evaluating its severity. It should integrate qualitative, semi-quantitative, and quantitative parameters. There is an agreement of the thresholds for the severity of primary MR but there is a debate concerning secondary MR: ESC/EACTS guidelines still use an effective regurgitant orifice area >20 mm2 and regurgitant volume >30 ml while the ACC/AHA 2017 guidelines update moved to the same thresholds for both types of MR, i.e., 40 mm2 and 60 ml, respectively. This discordance is part of the explanation of the fact that >75% of cardiologists in the survey appropriately quantified primary MR but only 44% recognised secondary MR as severe [30]. Both sets of guidelines acknowledge that further trials are needed to evaluate these thresholds which are based on their prognostic value more than on haemodynamics, Anyway, it is of the utmost importance to evaluate the severity of secondary MR only when the patient receives full medical treatment. Similarly, in secondary MR of ischaemic origin, when making the decision about the need for valve surgery, the severity of MR should be assessed at rest and not in the operating room where loading conditions are different.
Besides severity, echocardiography must identify Carpentier’s triad - lesions-aetiology- dysfunction - which will be essential for the choice of the most appropriate intervention.
It is also critical to assess the other valves, in particular the tricuspid valve, and evaluate the consequences of MR on the LA, LV, and pulmonary circulation as well as the right ventricular function, all being important factors for the choice of intervention and prognosis.
Transoesophageal echocardiography (TOE) is useful before surgery if TTE is suboptimal. On the other hand, TOE is needed to select the candidates for percutaneous interventions.
In addition to patient selection, echocardiographic monitoring is mandatory to guide transcatheter interventions and evaluate the immediate results of surgical and transcatheter valve interventions.
Stress tests
Stress tests should largely be performed in case of doubt in patients who claim to be asymptomatic. Stress echocardiography could be of interest in secondary MR when there are doubts about the severity and consequences of MR.
Cardiac magnetic resonance
A number of studies have advocated the use of cardiac magnetic resonance (CMR) to quantify the severity of MR, mainly because it is more reproducible than echocardiography. Its use should currently be limited to cases where echocardiography is not conclusive, because of the low level of evidence available today about the prognostic value of CMR-derived parameters and also costs and accessibility.
Computed tomography
Computed tomography (CT) is indicated in patients with calcification of the mitral annulus and before considering transcatheter annuloplasty, implantation of a valve, for sizing of the devices and for evaluating the risk of LV outflow track obstruction.
Viability testing
Viability testing, using echocardiography, radionuclide or CMR could be useful preoperatively if concomitant bypass surgery is considered.
Decision making and treatment
Decision making and treatment are optimally carried out in a valve centre including cardiology and surgery departments where a Heart Team (HT) is able to propose all the therapeutic alternatives with good efficacy and safety. The actual performance of these centres in terms of safety and rate of successful and durable repair is more important than arbitrary thresholds of activity, even if higher volumes are often related to better outcome.
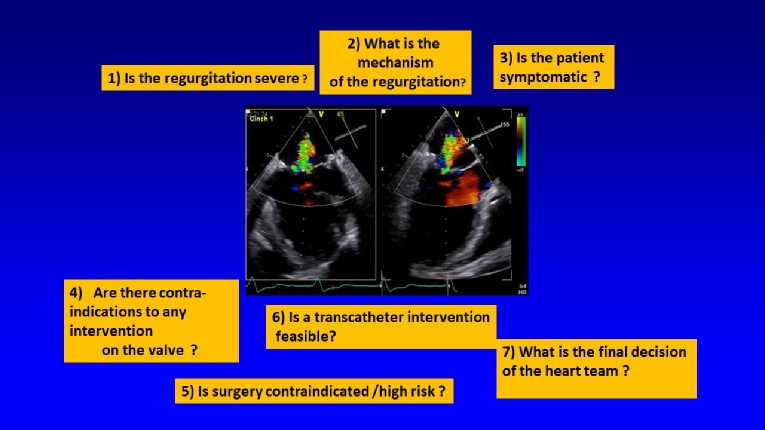
The Figure 1 illustrates the main step of the decision-making process.
Figure 1. Main steps for the management of mitral regurgitation.
Medical therapy
The survey showed that medical therapy is “overused” in primary MR where it has virtually no role if intervention is doable, and “underused” in secondary MR where guideline-directed medical therapy (GDMT), including cardiac resynchronisation therapy (CRT) when indicated, should be the first step of the treatment [30]. The efficacy of the medical treatment should be carefully evaluated and intervention considered early in case of failure.
The recent ESC/EACTS guidelines allowed the use of the new oral anticoagulants in patients with MR and atrial fibrillation [27]. Observation consistently shows that surgery is underused in MR [30,31].
Surgery
During surgery, the conventional approach using sternotomy is the most widely used worldwide. Minimal access approaches are increasingly adopted. Robotic surgery may represent a step forward but currently has a limited use. These new approaches have not proved to be superior to conventional surgery on hard endpoints.
In primary MR, the benefits of surgery are clearly established. Valve repair is preferable when a durable repair can be expected. As stated in the guidelines, “indication for intervention will be guided by the presence of symptoms and risk stratification that includes the assessment of ventricular function and size, atrial fibrillation, systolic pulmonary pressure and LA size. The role of surgery in asymptomatic patients in patients with normal LV function and size who are in sinus rhythm and have normal pulmonary pressures is still a matter of debate”. In such patients the decision will be individualised based on the patient’s condition and the likelihood of durable repair. The impact of earlier markers of LV dysfunction, such as longitudinal strain or biomarkers, on postoperative outcomes requires further research.
In secondary MR the spontaneous outcome is poor and related to the severity of MR and LV dysfunction. The potential impact of surgery on survival remains to be established. A recent randomised controlled trial (RCT) suggested that adding mitral repair to coronary artery bypass grafting (CABG) in patients with moderate MR (according to the ACC/AHA guidelines) neither improves LV remodelling nor provides survival benefit. Another trial compared valve repair to valve replacement using the same endpoint and was also negative, showing a high incidence of recurrence of MR in the repair group [32,33]. These trials are important; however, their conclusions are partially flawed by the non-clinical nature of the main endpoint (LV remodelling) and the lack of precision on the surgical techniques used.
The ESC/EACTS guidelines recommend valve surgery in patients with severe MR who undergo CABG and in those who have a low surgical risk where revascularisation is not considered who remain symptomatic despite GDMT. Valve repair is still often preferred but replacement should be considered in patients with unfavourable characteristics for repair. This statement is different from the ACC/AHA guidelines where valve replacement is preferred based on the trial cited before [33].
In cases with combined secondary tricuspid regurgitation, adding a tricuspid repair, if indicated, during left-sided surgery does not increase operative risk and has been demonstrated to provide reverse remodelling of the RV and improvement of the functional status even in the absence of substantial tricuspid regurgitation when annulus dilatation is present. It should therefore be performed liberally.
Transcatheter mitral valve intervention
Transcatheter mitral valve intervention was introduced more than 10 years ago, but it is less advanced than transcatheter aortic valve implantation (TAVI), mostly because of the complexity of the mitral valve.
The MitraClip technique aims at replicating the surgical edge-to-edge technique, creating a “double-orifice” mitral valve. This technique has been used in over 70,000 patients worldwide, two thirds having secondary MR. This represents by far the largest experience available in the domain of transcatheter mitral valve interventions.
Up until now, evidence was based on one randomised clinical trial (EVEREST II), including a mix of patients with primary and secondary MR and a number of registries including mostly, but not exclusively, patients with secondary MR. They showed that: i) in experienced centres MitraClip is a safe procedure with a low rate of complications; ii) it is effective in reducing MR with a very high procedural success; iii) it improves symptoms and quality of life; and iv) we remain uncertain about its effects on mortality outcomes.
In patients with primary MR, both sets of guidelines stated that the technique may be considered in high-risk patients with primary MR. However, there are differences concerning secondary MR. The 2017 ESC/EACTS Guidelines state that “When revascularisation is not indicated and surgical risk is not low, a percutaneous edge-to-edge procedure may be considered in patients with severe secondary MR who remain symptomatic despite GDMT, who have a suitable valve morphology by echocardiography, avoiding futility”. In the USA, the technique is not approved for clinical use for this indication.
The existing evidence suffers from the inherent limitations of registries, and prospective randomised controlled trials are required.
Fortunately, two RCTs, MITRA-FR and COAPT, were reported a few weeks ago and bring important, even if apparently contradictory, information [34,35]. These RCTs only included patients with secondary MR and for the first time compared GDMT with GDMT + MitraClip implantation.
Improvement in clinical outcomes was the primary endpoint of both trials: death or heart failure (HF) rehospitalisations at 12 months in MITRA-FR, and all HF hospitalisations at 24 months in COAPT. There were no differences between groups in MITRA-FR while the MitraClip reduced the rate of HF hospitalisations, and improved survival, quality-of-life and functional capacity in COAPT. The striking differences between the outcomes in the two trials are difficult to explain. The most likely explanation is that the patients in MITRA-FR were treated at a more advanced stage of the disease, with less initial MR, where the role of LV dysfunction predominates on the valve dysfunction.
In practice, before further analysis of the data and a potential update of the guidelines can be made, these results plead in favour of an early detection of secondary MR and referral to a heart valve centre where GDMT will be started. If symptoms remain, intervention may be considered if there is not too advanced cardiomyopathy, suggested by NYHA Class IV, severe LV dilatation, very low LV ejection fraction, RV failure, and severe tricuspid regurgitation.
In the other patients, LV assist/transplantation should be discussed by the Heart Team when appropriate. Finally, patients in whom no benefit can be expected from any intervention should stay on GDMT.
The other transcatheter techniques are at a more preliminary stage of evaluation and have bene evaluated in registries in a total of less than 3,000 patients.
In brief:
Transcatheter coronary sinus annuloplasty is relatively easy to perform; however, its efficacy seems limited.
Direct annuloplasty via transseptal approach, which mimics surgical annuloplasty, is a more demanding procedure but seems effective.
Chordal implantation through a transapical approach has shown promising results in selected patients with P2 prolapse.
A combination of techniques has been used in only a very limited number of patients.
Transcatheter valve implantation in native mitral valve disease is at an even earlier stage than repair since the largest experience is in <100 patients. The large size of the devices obliges the use of a transapical approach in most cases. Short-term results seem to be good in selected patients.
Because of the limited experience with transcatheter valve replacement, it is at present difficult to compare transcatheter repair and replacement, but it is likely that the two techniques will be complementary as is the case in surgery.
Thus, despite all progresses done, many challenges remain in the management of MR (Table 1).
Table 1. Challenges in the management of mitral regurgitation.
| Challenges in the management of mitral regurgitation. |
- Epidemiology of MR, especially secondary MRThresholds to define severity in secondary mitral regurgitation |
- Role of any intervention in the treatment of secondary mitral regurgitation |
- Indications for surgery in asymptomatic primary MR |
| - Efficacy and durability of MitraClip for treatment of high-risk patients and intermediate-risk patients with primary mitral regurgitation |
| - Feasibility and effectiveness of transcatheter mitral annuloplasty/chordal replacement techniques |
| - Feasibility and effectiveness of combination of transcatheter repair techniques |
| - Feasibility and effectiveness of transcatheter mitral valve replacementManagement of associated tricuspid regurgitation |
Mitral stenosis
Although the prevalence of rheumatic fever has greatly decreased in Western countries, mitral stenosis (MS) still results in significant morbidity and mortality worldwide. A new entity is emerging in Western countries - degenerative calcific mitral valve disease - which is mainly encountered in elderly patients and may be associated with massive mitral annular calcification (MAC).
Evaluation
Feasibility of percutaneous mitral commissurotomy (PMC)
Two-dimensional (2D) TTE usually provides sufficient information for routine management of MS. Valve area using planimetry is the reference measurement for severity and should be combined with measurements of mean transvalvular gradient and pulmonary pressures to assess the haemodynamic consequences of MS. The assessment of the feasibility of PMC must include the evaluation of valve pliability and degree of calcification, subvalvular apparatus thickening, and the commissural areas which benefit most from the use of three-dimensional (3D) echo. The existence of commissural fusion is mandatory before considering PMC, while the presence of calcification in one commissure is a risk factor, and in both commissures a contraindication for the technique. Finally, the absence of commissural fusion which can be observed in degenerative MS, after previous commissurotomy or in rare causes such as lupus, is a contraindication for PMC. The echocardiographic scores are useful and should be integrated in global scores including clinical variables [36]. These scores must be refined to predict the occurrence of MR.
TOE should be performed the day before PMC to exclude LA thrombus or after an embolic episode.
Stress testing
Stress testing is indicated in asymptomatic patients or if symptoms are equivocal or discordant with the severity of mitral MS. The additional value of stress echocardiography is not clearly demonstrated except if it shows a rapid rise in gradient and pulmonary pressures.
Computed tomography
CT is the best method to evaluate the location and severity of annular calcification.
Decision making and treatment
Medical therapy
Medical therapy is only palliative in patients with severe MS. Patients with moderate to severe MS and persistent atrial fibrillation should not receive novel oral anticoagulants (NOACs).
Cardioversion is not indicated before intervention in patients with severe MS, as it does not durably restore sinus rhythm. If atrial fibrillation is of recent onset and the LA only moderately enlarged, cardioversion should be performed soon after successful intervention. Catheter ablation of atrial fibrillation is not indicated in severe MS.
Prevention of rheumatic fever is key in countries where it is endemic in order to prevent MS but also after diagnosis and intervention.
Percutaneous mitral commissurotomy
PMC is now the default procedure in patients with MS because of the good results available beyond 20 years [36]. Because of the low frequency of MS in Western countries, the performance of PMC should ideally be performed in expert centres. Echocardiography plays an important role in monitoring the results during PMC.
In general, the indication for intervention should be limited to patients with clinically significant MS (valve area <1.5 cm2). However, PMC may be considered in symptomatic patients with a valve area >1.5 cm2 if symptoms cannot be explained by another cause and if the anatomy is favourable.
Intervention should be performed in symptomatic patients. Most patients with favourable valve anatomy currently undergo PMC. In patients with unfavourable anatomy, the choice of technique is still debated and must take into account the multifactorial nature of predicting the results of PMC. PMC will be favoured as an initial treatment for selected patients with mild-to-moderate calcification who have otherwise favourable clinical characteristics. Surgery, which is mostly valve replacement, is indicated in the other patients.
Asymptomatic patients, as assessed using stress testing, undergo PMC only if there is increased risk of systemic embolism or haemodynamic decompensation.
The most important contraindication to PMC is LA thrombus.
Some specific situations deserve discussion
During pregnancy, PMC can be performed after 20 weeks of pregnancy in symptomatic patients.
In patients with restenosis after surgical commissurotomy or PMC, PMC can be proposed in selected candidates with favourable characteristics if the predominant mechanism is commissural refusion.
The elderly population with rheumatic MS has a high risk for surgery and PMC is a useful option, even if only palliative. In elderly patients with degenerative MS and massive mitral annular calcification, surgery is very high risk. If degenerative mitral stenosis is severe, preliminary experience has suggested that transcatheter valve implantation of an inverted TAVI bioprosthesis in the mitral position is feasible in symptomatic elderly patients who are inoperable if the anatomy is suitable [37].
In patients with severe MS and moderate aortic valve disease, PMC can be performed to postpone the surgical treatment of both valves.
Finally, when MS is associated with severe tricuspid regurgitation, PMC may be considered in selected patients with sinus rhythm, moderate atrial enlargement, and functional tricuspid regurgitation secondary to pulmonary hypertension. In other cases, surgery on both valves is preferred [27].
Combined mitral stenosis and regurgitation
There is a lack of data on combined valve diseases. This does not allow evidence-based recommendations.
The aetiology is almost exclusively of rheumatic origin.
The general principles for its management are as follows:-
- When either stenosis or regurgitation is predominant, management follows the recommendations concerning the predominant VHD.
- When the severity of both stenosis and regurgitation is balanced, indications for interventions should be based on symptoms and on a global assessment of the consequences of the different valve lesions (i.e., symptoms or presence of LV dilatation or dysfunction, pulmonary hypertension).
- Valve replacement is preferable to repair in most cases.