















Overview of Cardiac Rehabilitation - Part 1
Derived from 'Country of the month' reports (comparison by topics)
The Patient
For whom is Cardiac Rehabilitation (CR) indicated?
Which categories of patients?
A majority of patients after acute myocardial infarction (AMI), percutaneous coronary intervention (PCI) or cardiac surgery are offered CR (high referral rates in countries such as France, Belgium and Bosnia and Herzegovina) but CR services to heart failure patients are severely underused across Europe, although there are some good practices (France, Belgium, Italy)
Ways of referral:
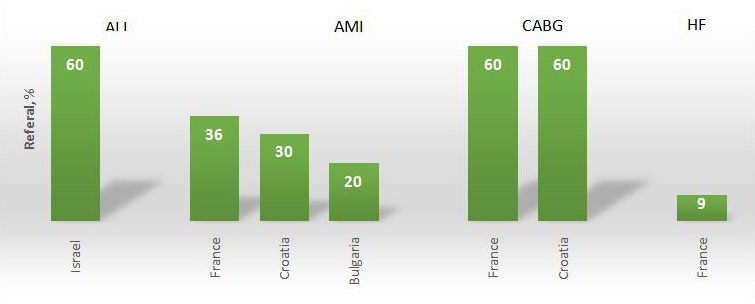
Patients are usually referred following a cardiologist assessment from either the discharging cardiac hospital, hospital-based clinics, community cardiologists or primary care physicians. France seems to be the only member that adapted standardized referral by an automatic software. France’s strategy accounted for a referral rate of 36% after AMI, 60-70 % after cardiac surgery, and 9 % after a first hospitalisation for Heart Failure. Bosnia and Herzegovina claimed that 60% of patients after an AMI, PCI or cardiac surgery are being referred down the line. Belgium reported that 78% of patients aged < 80 years who were hospitalized for a coronary event were advised to follow CR.
Referral rate:
The general referral rates vary strongly across Europe (figure 1).
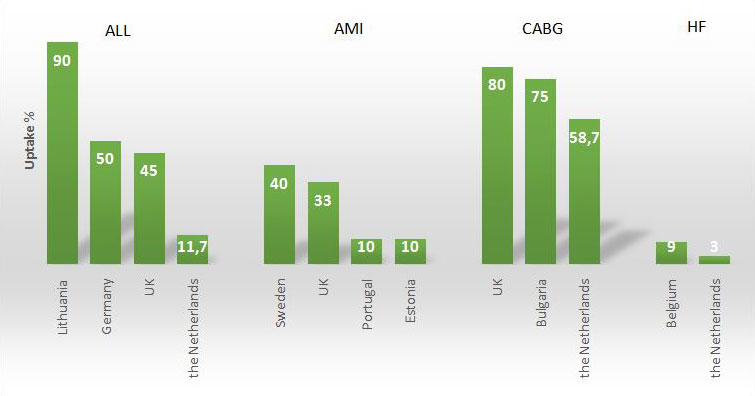
Uptake:
The general uptake rates vary strongly across Europe (figure 2).
The programme
Which Cardiac Rehabilitation (CR) programme is provided?
Which components
The description of phase II components differs little between the countries:
- supervised exercise sessions with graduated circuit training
- educational programs including smoking cessation
- risk factor management
- food and physical activity counseling
- psychosocial support
Some examples are: The Netherlands, Egypt, Italy
Type of physical training
Exercise training in patient groups remains the cornerstone of most CR programmes.
In Israel, some centres have added sessions of respiratory muscle training, Tai Chi and Yoga.
In the United Kingdom many programmes also offer individual, home-based rehabilitation such as the Heart Manual programme for those not wishing or unable to attend group programmes, and more recently evidence has demonstrated the utility of web-based cardiac rehabilitation.
Length
The outpatient programme duration varies between countries:
- some provide short programmes lasting 3-4 weeks (Germany, Latvia, Russia, Slovakia,
- Italy and Bosnia and Herzegovina)
- others have programmes of 6-12 weeks (Malta, The Netherlands, France, Ireland and Sweden)
- a few have programmes exceeding 12 weeks (Estonia, Poland and Egypt)
The Team
By whom is the Cardiac Rehabilitation (CR) programme conducted?
Team structure
The multi-disciplinary structure of the CR team (usually comprising a physician, nurse, physiotherapist, dietician, psychologist and social worker) is relatively consistent across all countries with some differences:
Cardiologists are usually programme coordinators (Israel, Ireland, Russia, Portugal, Spain, Bosnia and Herzegovina, Belgium and France), but even rehabilitation specialists may take the lead (Estonia, Portugal and Bosnia and Herzegovina). In several countries nurses and/or physiotherapists are in charge (United Kingdom, Sweden, Malta, Greece).
In Israel, Egypt, Portugal, United Kingdom, and Greece an exercise physiologist/masters may be welcomed to the phase II team working in team with the physiotherapists. On the contrary, phase II exercise classes in Ireland, Poland, Lebanon, Spain, Malta, Italy and Belgium are only run by physiotherapists
Education
Although Cardiac Rehabilitation (CR) is strongly recommended by the 2016 European Guidelines on CVD Prevention in Clinical Practice there are few recommendations for formal education of the CR team members.
Countries like Belgium , France, Italy and United Kingdom demand specific targeted CR education for the staff but so far only Spain includes CR in the training of young doctors.
Guidelines
In general, the European Guidelines on CVD Prevention in Clinical Practice are applied, but several countries have specific national guidelines: Belgium , France, Estonia, Israel, Italy and Slovenia.
British and American guidelines are less commonly used (United Kingdom, Malta, Lebanon).
The Centre
Where is the Cardiac Rehabilitation (CR) programme offered?
Format
In general, hospital-linked or healthcare-linked CR programmes are more commonly used in the Western and Northern part of Europe, programmes at specialised institutions are more widespread in the Eastern countries, whereas Southern European countries provide both alternatives.
Out-patient model
In the majority of the reporting countries, phase II was available only as an outpatient service. Well described examples can be found in Ireland, Portugal, Malta, Slovakia, Italy, United Kingdom and Belgium.
In-patient model
In Iceland and Germany, both inpatient and outpatient options are available according to patients’ preference, whereas in France and Croatia inpatient rehabilitation is only offered to post-surgical or high-risk patients in particular. Mainly in-patient models are reported from Poland, Latvia, Lithuania, Kazakhstan and Russia.
CR at home
With the assistance of telephone and/or computer monitoring programmes have been designed for CR at home (United Kingdom, Lithuania and Belgium) but this option is still fairly uncommon.
The Outcome
What is the quality and what are the costs?
Cost for patients, reimbursement
In most countries CR is provided within the framework of national or regional health services. There are countries with a significant number of privately-run centres, mainly in the Mediterranean zone (Portugal, Spain, Italy and Croatia).
Reimbursement varies, depending on the indication for CR: acute coronary syndromes and after percutaneous coronary intervention (PCI) are usually covered by all. The costs are covered by national health services and insurance companies, however in several countries even the patients must contribute (figure 3):
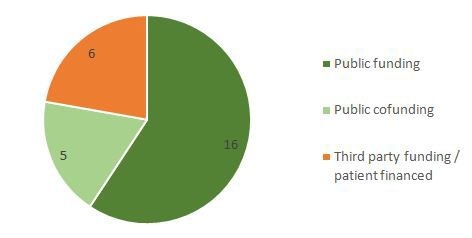
Public funding
Israel (public and private venues)
Ireland (public venues)
Latvia (inpatient)
Slovakia (specific indications)
Italy (public and private venues)
Croatia (specific indications)
Belgium (reimbursement for capped maximum number of sessions)
Portugal (public venues)
Public co-funding
Estonia (if < 6 months post AMI)
Sweden (if > high cost protection)
Latvia (outpatient)
Third party funding/Patient financed
The Netherland (cardiologist referral)
Slovakia (specific indications)
Lebanon (exclusively paid by patients)
Greece (mostly private)
Croatia (specific indications)
Audit and quality control
Certain countries have implemented specific accreditations attesting whether CR centres meet minimum standards. In Belgium an audit is under way for quality control in several CR centres to be published in 2017.
In The Netherlands, each 3 months participating clinics receive periodic feedback on quality indicators accompanied by an educational outreach visit. Similar efforts are made in France and the United Kingdom.
Surveys and databases
Periodic national surveys on centre distribution, disease epidemiology, patient demographics and outcomes data have been informative in many countries (Turkey, United Kingdom, Portugal, Spain, Poland, Italy, Greece, Belgium and France).
Electronic database registries are being increasingly applied throughout Europe: Sweden (SWEDEHEART), Spain (R-EUReCa),The Netherlands (CARDSS study group) and the United Kingdom (NACR).
Israel has recently developed a similar platform but just for heart failure patients. These models are expected (or have shown already!) to increase adherence with the guideline-recommended therapeutic decisions, support patient management, data archiving and quality assessment for CR.
The Future
Plans for the future
Obstacles
Some common health system-related obstacles reported were:
- Insufficient availability of beds and ambulatory facilities (Portugal, France)
- Lack of funding (Latvia, Egypt, Lebanon, Portugal, Greece)
- Uneven geographical distribution of CR centres (Portugal, Spain)
Some professionals-related obstacles were also described, namely:
- Small community CR not routinely being practiced (Israel)
- Insufficient adherence to the guidelines related to professional knowledge and attitude (The Netherlands, Portugal, United Kingdom)
- Insufficient number of cardiopulmonary physiotherapists available (Turkey)
Patient-related obstacles included fear of prolonged absence from work (Germany, Portugal) and poor patient motivation (Portugal, United Kingdom).
Strategies for Secondary Prevention and CR
Innovative solutions for the future proposed in the action plans included:
- The use of CR delivery as an established national health system quality indicator (Israel)
- referral of non-classical CR indications (Israel)
- risk factor counselling reimbursement by insurance companies (Germany)
- continued reinforced intervention up to 3 years after rehabilitation (Italy)
- development of web-based programs (The Netherlands)
- establishment of individualized models of CR (Sweden)
- setup of an educational programme for pupils and their parents (Portugal)
- centre certification to incorporate improvement in exercise capacity/risk reduction outcomes (United Kingdom)
- the support of lagging programmes by the top performing programmes (France)
- frailty tailored CR programs (Challenges in secondary prevention after acute myocardial infarction: A call for action) (1).
In fact, in the framework of the ESC Prevention of CVD Programme, which is led by the EAPC in collaboration with ACCA and ACNAP, a consensus document "Challenges in secondary prevention after acute myocardial infarction: A call for action" (1) was recently published in which some of the existing gaps for secondary prevention strategies were reviewed and effective interventions/innovative strategies in relation to the patients, healthcare providers and healthcare systems were endorsed.
Overview of Cardiac Rehabilitation - Part 2
To access part 2, go to:
Previous page
Note: The content of this article reflects the personal opinion of the author/s and is not necessarily the official position of the European Society of Cardiology.