

















What is the quality and what are the costs?
Cost for patients, reimbursement
In most countries CR is provided within the framework of national or regional health services. There are countries with a significant number of privately-run centres, mainly in the Mediterranean zone (Portugal, Spain, Italy and Croatia).
Reimbursement varies, depending on the indication for CR: acute coronary syndromes and after percutaneous coronary intervention (PCI) are usually covered by all. The costs are covered by national health services and insurance companies, however in several countries even the patients must contribute (figure 3):
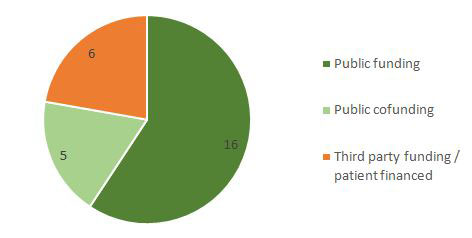
| Public funding | Public co-funding | Third party funding/Patient financed |
|---|---|---|
| Israel (public and private venues) | Turkey | The Netherlands (cardiologist referral) |
| Ireland (public venues) | Estonia (if < 6 months post AMI) | Slovakia (specific indications) |
| Bulgaria | Sweden (if > high cost protection) | Lebanon (exclusively paid by patients) |
| Poland | Latvia (outpatient) | Slovenia |
| Latvia (inpatient) | Egypt | Greece (mostly private) |
| Lithuania | Croatia (specific indications) | |
| Russia | ||
| Malta | ||
| Slovakia (specific indications) | ||
| Italy (public and private venues) | ||
| Bosnia and Herzegovina | ||
| Croatia (specific indications) | ||
| Belgium (reimbursement for capped maximum number of sessions) |
||
| France | ||
| Germany | ||
| Portugal (public venues) |
Audit and quality control
Certain countries have implemented specific accreditations attesting whether CR centres meet minimum standards. In Belgium an audit is under way for quality control in several CR centres to be published in 2017.
In The Netherlands, each 3 months participating clinics receive periodic feedback on quality indicators accompanied by an educational outreach visit. Similar efforts are made in France and the United Kingdom.
Surveys and databases
Periodic national surveys on centre distribution, disease epidemiology, patient demographics and outcomes data have been informative in many countries (Turkey, United Kingdom, Portugal, Spain, Poland, Italy, Greece, Belgium and France).
Electronic database registries are being increasingly applied throughout Europe: Sweden (SWEDEHEART), Spain (R-EUReCa),The Netherlands (CARDSS study group) and the United Kingdom (NACR).
Israel has recently developed a similar platform but just for heart failure patients. These models are expected (or have shown already!) to increase adherence with the guideline-recommended therapeutic decisions, support patient management, data archiving and quality assessment for CR.
Note: The content of this article reflects the personal opinion of the author/s and is not necessarily the official position of the European Society of Cardiology.