

















Case Presentation
A 45-year-old Caucasian male presents to his general practitioner for medication review having recently had a successful ablation for symptomatic paroxysmal atrial fibrillation. His CHA2DS2Va score is 0 and he stopped his oral anticoagulant a few months after his ablation.
He is concerned about his overall ‘heart health’ as his father was diagnosed with angina in his late 50s. There is no other family history of cardiac issues. He is a non-smoker, avid cyclist with a BP in clinic of 124/82mmHg and drinks alcohol minimally. A standard lipid profile shows a total cholesterol of 4.1mmol/L, HDL of 1.0mmol/L, LDL of 2.2mmol/L and triglycerides of 0.9mmol/L. He is 1.8m tall with a weight of 80kg giving a BMI of 24kg/m2. Previous echocardiography was normal and his ECG in clinic is also normal showing sinus rhythm.
What calculators might you use to advise him on his cardiovascular risk?
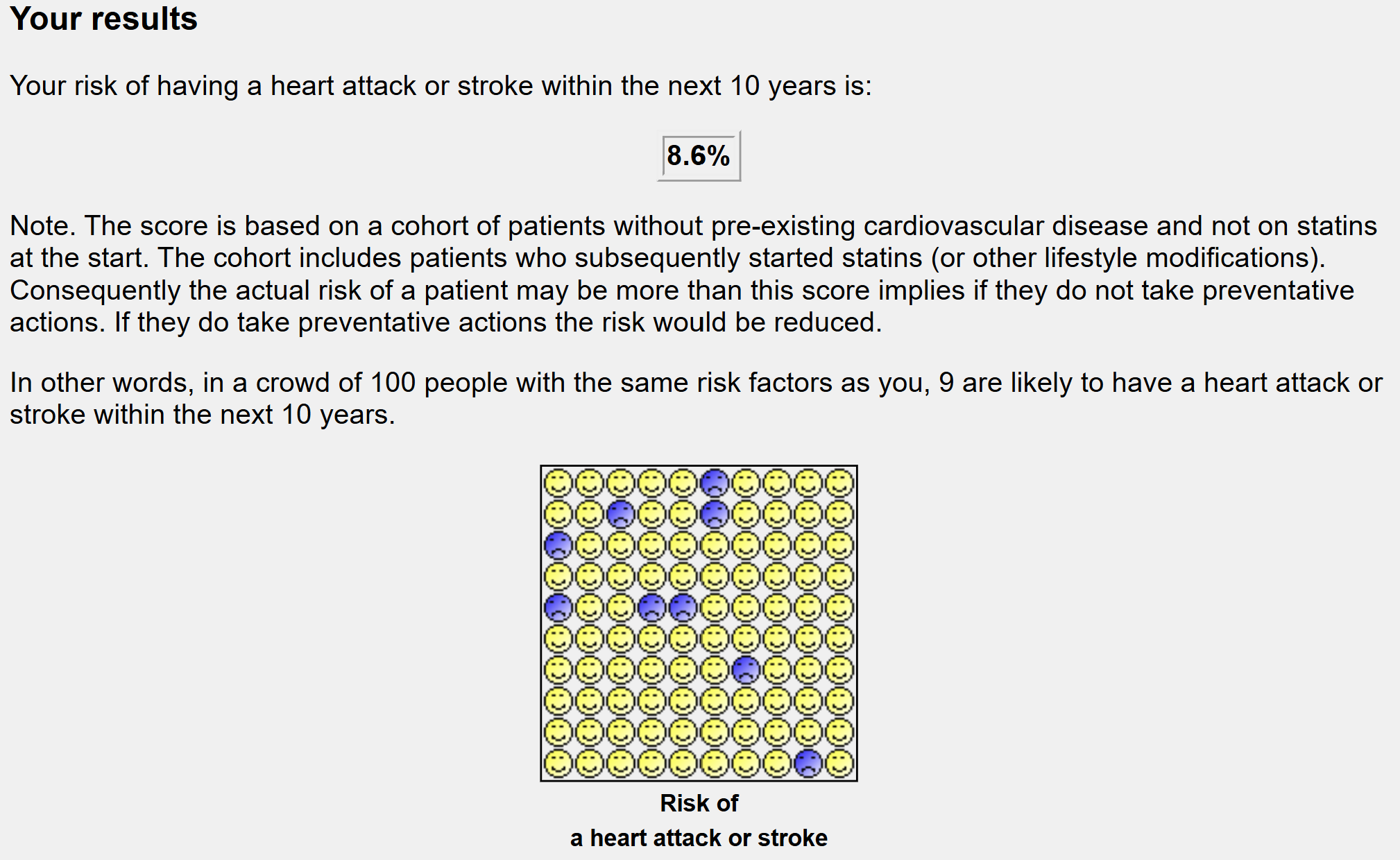
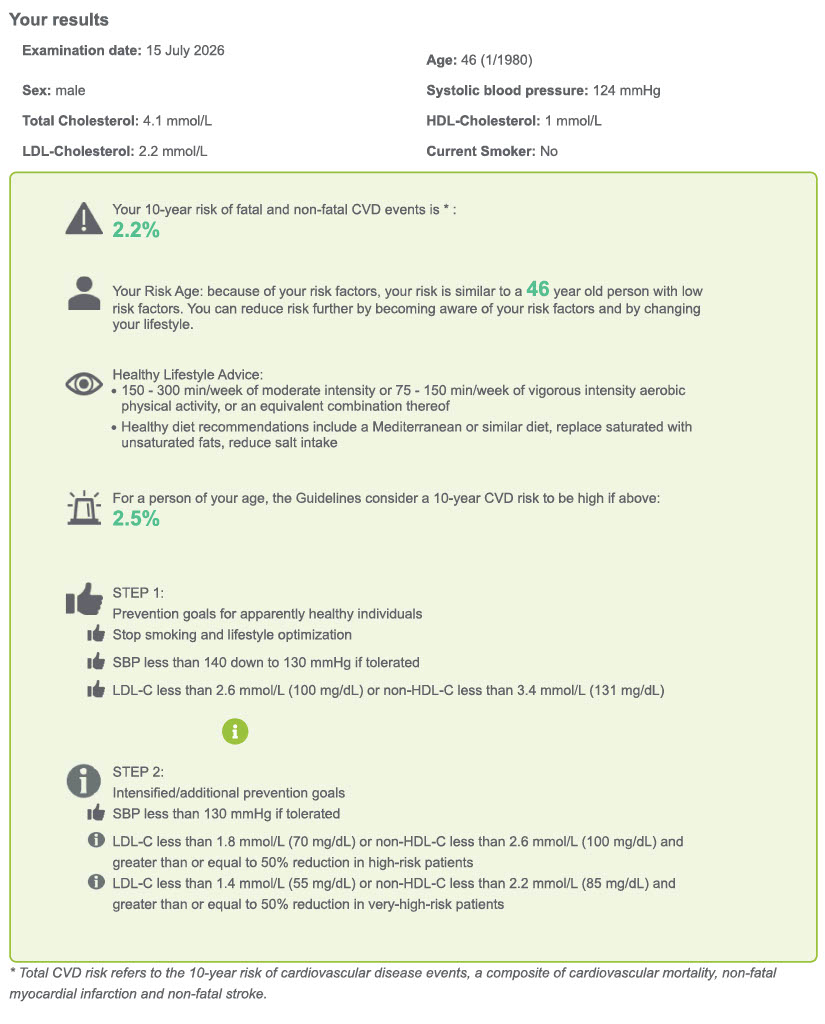
The ESC 2025 focussed update initially recommends use of the SCORE2 algorithm for a low-risk country (United Kingdom). Entering his data yields a 10-year CVD risk of 2.1%, with a guideline of threshold of treatment to be 2.5%. Within the National Health Service, the National Institute of Clinical Excellence (NICE) recommends the QRISK3 score to calculate a 10-year risk of threshold of treatment for CVD events which gave a value of 8.6% (threshold for treatment 10%).
The SCORE2 algorithm does not take into account ‘risk modifiers’ which are outlined in the ESC focussed update. ESC guidelines would suggest considering the patient’s family history as a strong risk modifier, but would still not recommend treatment based on his LDL alone (2.2mmol/L is well below ESC thresholds for treatment in low-risk individuals), focussing on lifestyle advice. The ESC Focused Update discusses risk modifiers of biomarkers of a persistently elevated hs-CRP as well as an elevated Lp(a) as well as the relevance of coronary artery calcium scores to emphasise lifetime risk, not just 10-year risk in younger patients. The QRISK3 score has other modifiers incorporated within the questionnaire - in his case of relevance for family history of CVD <60years old as well as atrial fibrillation.
Are there any indications for routine genetic testing?
There are no indications for genetic testing for dyslipidaemia based on his current presentation. However, the patient went and had a commercially available CVD polygenic risk score measured. Here, the polygenic risk reflects aggregate common variant risk and is independent of traditional risk factors. It captures lifelong exposure to atherogenic risk, which may not yet be phenotypically expressed.
This found a risk score in the 81-90 range (see report) suggesting that 80% of individuals had an overall lower genetic risk than this patient and around 10% had a higher overall genetic risk than this patient.
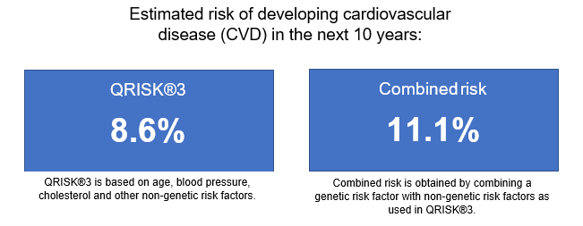
This was incorporated alongside his QRISK3 score and presented as a CVD integrated risk tool suggesting a 10-year risk of CVD above 10% and the treatment threshold for primary prevention.
With the above in mind, primary prevention with statin treatment was initiated as the patient felt no further applicable lifestyle measures were remaining for him to modify and he wished to reduce his longer-term risk.
This case illustrates how polygenic risk scores may act as a risk enhancer in individuals with low short-term cardiovascular risk but potential for elevated lifetime risk. In this patient, polygenic risk information did not replace established risk calculators, but provided additional context beyond traditional risk factors and family history, supporting shared decision-making around primary prevention. While polygenic risk scores are not yet incorporated into guideline-endorsed algorithms, their increasing availability highlights the need for clinicians to understand their appropriate interpretation, limitations, and potential role in personalised cardiovascular risk assessment.
Comments
This is a clear, clinically relevant case illustrating how polygenic risk scores (PRS) might act as a risk enhancer in an individual with low short-term but potentially higher lifetime cardiovascular risk. The narrative is coherent, the clinical details are appropriate, and the discussion is well aligned with current guideline debates. The case is particularly valuable because it shows how PRS may influence shared decision-making rather than replacing standard risk tools.
