

















Keywords
Atherosclerosis; biomarkers; coronary artery disease; coronary imaging; inflammation
Abbreviation list
ACS: acute coronary syndrome
CAD: coronary artery disease
CCS: chronic coronary syndrome
FAI: fat attenuation index
hsCRP: high-sensitivity C-reactive protein
Take-home messages
Introduction
Coronary artery disease (CAD) remains the leading cause of cardiovascular morbidity and mortality worldwide despite major advances in lipid-lowering therapy, antithrombotic treatment, and coronary revascularisation [1,2]. Increasing evidence indicates that inflammation is not merely associated with atherosclerosis but actively contributes to endothelial dysfunction, plaque formation, plaque destabilisation, and thrombotic complications [1-5]. Persistent inflammatory activity is now recognised as an important contributor to residual cardiovascular risk, including in patients receiving guideline-directed preventive therapy [1,2,6,7].
Understanding of immune and inflammatory pathways involved in chronic and acute coronary syndromes has expanded considerably in recent years. The field has evolved beyond isolated inflammatory biomarkers towards integrated approaches combining circulating biomarkers, multimodality cardiovascular imaging, metabolic profiling, and emerging omics technologies [1,2,8-10]. Novel imaging techniques, including coronary computed tomography-derived assessment of perivascular inflammation, have further strengthened interest in inflammation-guided cardiovascular risk stratification, although their routine clinical role remains incompletely defined [9-11].
Therapies including colchicine and interleukin-targeted approaches have demonstrated potential cardiovascular benefit in selected populations, although uncertainties remain regarding patient selection, long-term safety, optimal inflammatory targets, and broader clinical application [3,4,12-15].
This review summarises contemporary concepts linking inflammation and CAD, with emphasis on mechanisms of vascular injury, clinically relevant biomarkers, advanced imaging approaches, and emerging therapeutic strategies. Particular attention is given to residual inflammatory risk, multimarker assessment, and current limitations of inflammation-targeted cardiovascular care.
Emerging mechanisms: inflammation as a central mediator of atherothrombosis
Inflammation plays a central role (Figure 1) in the initiation, progression, and clinical destabilisation of coronary atherosclerosis [1,2,4,5]. Endothelial dysfunction represents an early event characterised by oxidative stress, increased vascular permeability, and upregulation of adhesion molecules including vascular cell adhesion molecule-1 (VCAM-1) and intercellular adhesion molecule-1 (ICAM-1). These changes promote leukocyte adhesion, monocyte migration into the arterial wall, macrophage activation, and foam-cell formation following uptake of modified lipoproteins, ultimately contributing to the development of lipid-rich atherosclerotic plaques [1,2].
Figure 1. Inflammation in coronary artery disease: mechanisms, biomarkers, imaging, and therapeutic targets.
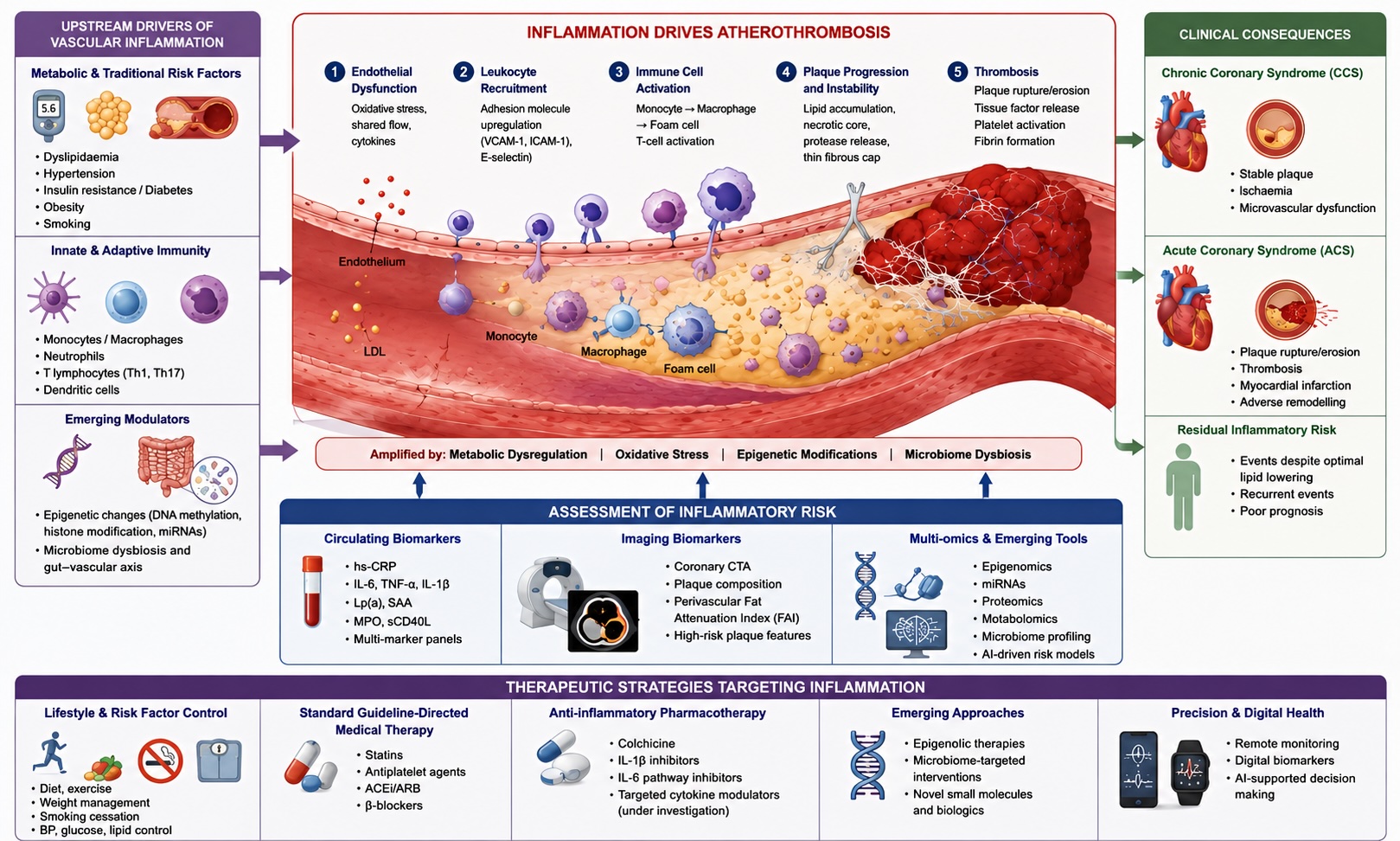
Schematic overview of the contemporary inflammatory paradigm in CAD. The figure illustrates the role of inflammation in endothelial dysfunction, leukocyte recruitment, immune-cell activation, plaque progression, and thrombotic complications contributing to chronic and acute coronary syndromes. Upstream drivers of vascular inflammation include traditional cardiovascular risk factors, metabolic dysregulation, innate and adaptive immune activation, epigenetic mechanisms, and microbiome-related pathways. The diagram summarises current approaches to inflammatory risk assessment using circulating biomarkers, cardiovascular imaging, and multi-omics technologies, including perivascular FAI assessment by coronary computed tomography angiography. Therapeutic strategies targeting inflammatory risk include lifestyle optimisation, guideline-directed medical therapy, colchicine, cytokine-targeted therapies, emerging epigenetic and microbiome-based interventions, and artificial intelligence-assisted precision cardiovascular approaches.
Pro-inflammatory cytokines, particularly interleukin-1β (IL-1β), interleukin-6 (IL-6), and tumour necrosis factor-α (TNF-α), amplify vascular inflammation through activation of endothelial and immune-cell signalling pathways [1,2,4,14]. Persistent cytokine activation promotes extracellular matrix degradation, fibrous cap thinning, apoptosis of vascular smooth muscle cells, and increased thrombogenicity, thereby enhancing susceptibility to plaque rupture and acute coronary syndromes [1,3,4]. Activation of the NLRP3 inflammasome has also emerged as an important upstream mechanism linking cholesterol crystal accumulation, innate immune activation, and cytokine-mediated vascular injury [1,2].
Metabolic abnormalities substantially influence inflammatory signalling in CAD. Insulin resistance, visceral adiposity, and metabolic syndrome are associated with chronic low-grade inflammation mediated through adipokine imbalance, oxidative stress, and the activation of innate immune pathways [1,2,6]. These mechanisms contribute to endothelial dysfunction, dyslipidaemia, impaired fibrinolysis, and persistent residual cardiovascular risk despite lipid-lowering therapy.
Epigenetic regulation has also attracted interest in atherosclerosis research. DNA methylation, histone modification, and non-coding RNA signalling influence inflammatory, metabolic, and vascular remodelling pathways and may partially explain interindividual variability in inflammatory responses [1,2]. In parallel, the gut and oral microbiomes have been implicated in vascular inflammation through immune modulation and production of pro-atherogenic metabolites, although these mechanisms remain incompletely characterised.
Inflammatory activity is clinically relevant across both chronic and acute coronary syndromes and has been associated with plaque instability, larger infarct size, adverse ventricular remodelling, recurrent ischaemic events, and worse long-term prognosis [1,2,16,17]. Emerging evidence further suggests that local vascular inflammation interacts with plaque morphology and coronary haemodynamics in determining clinical risk.
Recent advances in cardiovascular imaging have strengthened interest in the non-invasive assessment of coronary inflammation. Characterisation of perivascular adipose tissue (PVAT) and coronary computed tomography-derived fat attenuation index (FAI) has emerged as a promising approach for evaluating local inflammatory activity [9-11]. These techniques provide indirect assessment of coronary inflammation through detection of inflammatory changes within pericoronary adipose tissue and may offer incremental prognostic value beyond conventional anatomical plaque assessment. However, inflammatory imaging remains investigational and requires further standardisation and outcome-based validation before widespread implementation in clinical practice [9,10].
Biomarkers: from conventional inflammatory markers to multimarker and omics-based approaches
Biomarker assessment has become an important component of cardiovascular risk evaluation in CAD [1,2]. High-sensitivity C-reactive protein (hsCRP) remains the most extensively validated and clinically accessible marker of systemic inflammation in both primary and secondary prevention [6-8,18]. Elevated hsCRP levels are associated with increased risk of myocardial infarction, stroke, cardiovascular death, and recurrent ischaemic events, including in individuals without marked lipid abnormalities [6,7,18]. However, current evidence suggests that CRP primarily reflects upstream inflammatory activation rather than acting as a direct mediator of atherosclerosis [2,8].
Attention has increasingly shifted towards upstream inflammatory pathways, particularly interleukin-1β (IL-1β) and interleukin-6 (IL-6) signalling, which appear more directly involved in vascular inflammation and plaque destabilisation [1-3,14]. Elevated IL-6 concentrations have been associated with adverse cardiovascular outcomes and may provide incremental prognostic information beyond hsCRP alone [1,2,14]. Biomarkers reflecting thromboinflammatory activation, including fibrinogen and D-dimer, further illustrate the interaction between inflammation, coagulation, and thrombosis, particularly in acute coronary syndromes.
Multimarker risk stratification has gained increasing relevance in CAD [1,2]. Combined assessment of inflammatory activity, endothelial dysfunction, myocardial injury, lipid-related risk, and haemostatic activation may improve identification of patients at increased cardiovascular risk despite guideline-directed therapy [1,6]. Such approaches may be particularly relevant in patients with chronic coronary syndromes, diabetes mellitus, obesity, or recurrent ischaemic events, although standardised multimarker algorithms and clinically validated treatment thresholds remain limited.
Advances in molecular profiling technologies have expanded interest in omics-based cardiovascular risk assessment. Genomic, transcriptomic, epigenomic, proteomic, and metabolomic approaches provide systems-level characterisation of inflammatory and metabolic pathways involved in atherosclerosis [1,2]. Transcriptomic and epigenetic signatures may help identify individuals with enhanced inflammatory susceptibility, while proteomic analyses have identified candidate mediators associated with plaque instability, immune activation, and recurrent cardiovascular events. Nevertheless, translation of these approaches into routine clinical practice remains limited.
Non-coding RNA pathways, including microRNAs and circular RNAs, have emerged as potential regulators of endothelial function, macrophage activation, lipid metabolism, and inflammatory signalling. Similarly, metabolites derived from the oral and gut microbiota may contribute to vascular inflammation and atherogenesis [1,2]. These pathways remain areas of ongoing translational investigation.
Integration of circulating biomarkers with cardiovascular imaging has attracted increasing interest. Combination of hsCRP and other inflammatory markers with coronary artery calcium scoring, coronary computed tomography angiography (CCTA), plaque characterisation, and perivascular FAI may improve the identification of high-risk inflammatory phenotypes beyond conventional lipid-based assessment alone [9, 11]. Such multimodal approaches may further refine cardiovascular risk stratification, although additional prospective validation remains necessary before routine clinical implementation.
Therapeutic frontiers: anti-inflammatory strategies in coronary artery disease
Recognition of inflammation as a modifiable contributor to atherosclerotic cardiovascular disease has increased interest in targeted anti-inflammatory therapies [1,2,4]. Among currently investigated pathways, inhibition of the interleukin-1β (IL-1β)/interleukin-6 (IL-6) axis remains the most extensively studied strategy [3,14]. Experimental and clinical evidence suggests that suppression of cytokine-mediated inflammatory signalling may reduce plaque instability, attenuate vascular inflammation, and lower recurrent ischaemic risk independently of lipid reduction [1-4]. Clinical trials evaluating canakinumab, colchicine, anakinra, and IL-6 receptor antagonists have supported the concept of inflammation-targeted cardiovascular therapy, although treatment effects appear to vary according to patient selection, timing of intervention, baseline inflammatory burden, and clinical presentation [3,12-15].
Low-dose colchicine has emerged as the most clinically accessible anti-inflammatory strategy in chronic coronary disease and selected post-myocardial infarction populations [12,13,15]. However, uncertainties remain regarding optimal patient selection, duration of therapy, long-term tolerability, drug interactions, and the risk of infection or non-cardiovascular adverse events [1,2,4]. Similarly, selective cytokine inhibition has demonstrated biological efficacy but may be limited by cost, immunosuppressive effects, and safety concerns [3,14]. These observations support a more individualised approach to the identification of patients most likely to derive clinical benefit from anti-inflammatory therapy.
Beyond direct cytokine inhibition, several established cardiovascular therapies exert clinically relevant anti-inflammatory effects. Statins, angiotensin-converting enzyme inhibitors, sodium-glucose cotransporter-2 (SGLT2) inhibitors, glucagon-like peptide-1 (GLP-1) receptor agonists, and intensive cardiometabolic risk reduction strategies have all been associated with attenuation of inflammatory signalling pathways [1,2,6]. This overlap between metabolic regulation and immune modulation further supports the concept that cardiovascular risk extends beyond cholesterol lowering alone.
Emerging therapeutic approaches increasingly focus on upstream molecular regulators of vascular inflammation. Epigenetic modulation, including targeting of DNA methylation, histone modification, and chromatin remodelling, has demonstrated experimental potential to influence inflammatory gene expression and vascular remodelling, although these strategies remain largely preclinical [1,2]. Similarly, the microbiome-immune-vascular axis has attracted interest as a potential therapeutic target. Experimental data suggest that microbial metabolites and alterations in gut and oral microbiota composition may contribute to endothelial dysfunction, systemic inflammation, and plaque progression, although robust cardiovascular outcome data remain lacking.
Rapid advances in artificial intelligence, digital health, and multimodal data integration may further influence the management of inflammatory cardiovascular risk. Integration of omics technologies, circulating biomarkers, electronic health records, wearable-device data, and advanced cardiovascular imaging may facilitate more refined cardiovascular risk stratification and therapeutic selection. However, challenges related to explainability, data governance, algorithmic bias, and clinical implementation remain unresolved [1,2].
Inflammation-targeted cardiovascular prevention may be particularly relevant in systemic inflammatory disorders including rheumatoid arthritis and systemic lupus erythematosus, where accelerated atherosclerosis contributes to increased long-term cardiovascular risk [1,2]. Nevertheless, prospective evidence defining optimal screening strategies and therapeutic algorithms in inflammatory rheumatic diseases remains limited.
Imaging of coronary inflammation
Cardiovascular imaging has become increasingly important for non-invasive assessment of vascular inflammation and plaque vulnerability in coronary artery disease [1,2,9-11]. Unlike circulating biomarkers, which reflect systemic inflammatory activity, imaging modalities provide anatomical and tissue-level characterisation of local coronary inflammation. Current imaging approaches aim to identify inflamed, rupture-prone plaques, quantify inflammatory burden, and improve cardiovascular risk stratification beyond conventional assessment of luminal stenosis alone.
Coronary computed tomography angiography (CCTA) has emerged as the principal imaging modality for assessment of coronary inflammation in clinical and translational research [9-11]. In addition to evaluation of stenosis severity and plaque morphology, contemporary CCTA techniques permit characterisation of plaque composition, high-risk plaque features, and inflammatory changes within adjacent pericoronary tissues. Particular attention has focused on PVAT, which interacts dynamically with the vascular wall through bidirectional inflammatory signalling. Inflammatory activation of the coronary artery alters the biological properties of adjacent adipose tissue, resulting in measurable changes in computed tomography attenuation profiles [9,10].
The perivascular FAI has emerged as a promising imaging biomarker reflecting local coronary inflammatory activity [9,10]. FAI quantifies attenuation gradients within pericoronary adipose tissue and indirectly captures inflammation-related tissue remodelling surrounding coronary arteries. Elevated FAI values have been associated with increased cardiovascular risk, plaque vulnerability, and future adverse cardiovascular events independently of traditional risk factors and coronary calcium burden [9,10]. Integration of FAI with conventional plaque assessment may improve identification of high-risk coronary phenotypes and support more refined cardiovascular risk stratification.
Additional CCTA-derived inflammatory markers are also under investigation, including pericoronary adipose tissue density, plaque radiomics, low-attenuation plaque burden, positive remodelling, and napkin-ring morphology [9,11]. Combined assessment of anatomical plaque characteristics and inflammatory imaging biomarkers may provide a more comprehensive evaluation of plaque biology than luminal stenosis assessment alone. There is also increasing interest in integrating imaging findings with circulating biomarkers such as hsCRP and IL-6 to develop multimodal inflammatory risk models [1,2].
Several limitations currently restrict routine implementation of inflammatory imaging in clinical practice. Standardisation of acquisition protocols, reproducibility of FAI measurements, inter-vendor variability, and definition of clinically relevant thresholds remain incompletely resolved [9,10]. In addition, pericoronary adipose tissue composition differs across coronary segments and patient populations, complicating interpretation of attenuation values. Current evidence supporting inflammatory imaging remains largely observational, and prospective outcome-based studies demonstrating incremental therapeutic benefit are still limited.
Positron emission tomography (PET)-based imaging approaches, including ^18F-fluorodeoxyglucose (^18F-FDG) and ^18F-sodium fluoride (^18F-NaF) imaging, provide additional opportunities for visualisation of inflammatory and metabolic activity within atherosclerotic plaques [2,9]. However, widespread clinical application remains constrained by limited availability, radiation exposure, cost, and technical challenges related to myocardial tracer uptake in coronary imaging. Hybrid imaging modalities combining PET and cardiac magnetic resonance imaging may further improve tissue characterisation, although these techniques currently remain primarily research tools.
Inflammatory imaging should currently be regarded as complementary rather than definitive in cardiovascular decision-making. Existing evidence does not support the use of imaging-derived inflammatory markers as stand-alone determinants for initiation of anti-inflammatory therapy or invasive management strategies. Nevertheless, imaging of coronary inflammation remains a rapidly evolving field with potential implications for longitudinal assessment of therapeutic response and identification of patients with persistent inflammatory risk.
Integrative synthesis: a contemporary framework for inflammation in CAD
Inflammation provides a central mechanistic link between endothelial dysfunction, immune activation, metabolic dysregulation, thrombosis, and adverse cardiovascular outcomes in coronary artery disease [1,2,4,5]. Contemporary concepts of atherothrombosis extend beyond lipid accumulation alone and incorporate interactions among inflammatory signalling pathways, cardiometabolic factors, epigenetic regulation, and vascular remodelling.
The field has moved from reliance on isolated inflammatory biomarkers towards multimarker, multi-omics, and imaging-integrated approaches to better characterise residual inflammatory risk [1,2,6,8]. Integration of circulating biomarkers with advanced imaging modalities, including coronary computed tomography angiography and perivascular fat attenuation analysis, may provide a more comprehensive assessment of plaque vulnerability and inflammatory activity [9-11].
Anti-inflammatory therapeutic strategies, particularly colchicine and cytokine-targeted approaches, have shown encouraging but incomplete evidence regarding long-term cardiovascular benefit, safety, and optimal patient selection [3,12-15]. Epigenetic modulation, microbiome-targeted therapies, and artificial intelligence-assisted multimodal risk prediction may further contribute to precision cardiovascular medicine, although substantial translational and implementation challenges remain [1,2].
In current clinical practice, inflammatory risk assessment should complement established cardiovascular prevention strategies. Biomarkers and inflammatory imaging findings should be interpreted in relation to overall cardiovascular risk, clinical presentation, and comorbidities rather than applied uniformly across all CAD populations.
Practical implications and future research directions
Incorporation of inflammatory assessment into cardiovascular risk stratification represents an increasingly important component of CAD management [1,2]. Measurement of hsCRP together with conventional cardiovascular risk factors may assist in identifying patients with persistent inflammatory risk despite optimal guideline-directed therapy [6-8,18]. In selected high-risk populations, particularly those with established atherosclerotic cardiovascular disease, adjunctive anti-inflammatory strategies such as low-dose colchicine may be considered, while recognising the importance of individual assessment of tolerability, infection risk, and drug interactions [12,13,15].
The integration of circulating biomarkers with advanced cardiovascular imaging may further refine the identification of high-risk inflammatory phenotypes. Combined biomarker-imaging approaches using CCTA-derived plaque characterisation, perivascular fat attenuation analysis, and inflammatory biomarkers may improve risk discrimination beyond traditional lipid-centred assessment, particularly in patients with intermediate or uncertain cardiovascular risk profiles [9-11].
Several areas require further investigation before widespread implementation in routine practice. Large prospective trials are needed to better define the efficacy, safety, and optimal patient selection criteria for IL-1β, IL-6, and other inflammation-targeted therapies across diverse CAD phenotypes [3,14]. Additional studies are also required to validate integrated multi-omics and artificial intelligence-assisted risk prediction models capable of combining molecular, imaging, and clinical data into clinically applicable frameworks [1,2].
Emerging therapeutic approaches targeting epigenetic regulation and microbiome-related inflammatory pathways remain investigational and require further translational and clinical validation [1,2]. Inflammatory biomarkers and imaging findings should also be interpreted cautiously, as some markers may reflect downstream inflammatory burden rather than direct causal mechanisms of disease [2,8]. Recognition of phenotypic heterogeneity across chronic coronary syndromes, acute coronary syndromes, coronary microvascular dysfunction, and systemic inflammatory disorders will be important for the development of more individualised inflammation-guided cardiovascular strategies.
Patient-oriented message
Patients should be informed that coronary artery disease is influenced not only by cholesterol accumulation but also by chronic vascular inflammation, which may contribute to plaque instability and recurrent cardiovascular events even when standard therapies are optimised. Discussions should emphasise that inflammation represents one component of overall cardiovascular risk alongside blood pressure, cholesterol, diabetes, smoking, obesity, physical inactivity, and psychosocial stress. Clinicians should encourage adherence to guideline-directed medical therapy, lifestyle modification, weight management, regular physical activity, smoking cessation, and cardiometabolic risk control, while explaining that selected patients may additionally benefit from anti-inflammatory therapeutic strategies. The interpretation of inflammatory biomarkers or advanced imaging findings should remain individualised and considered within the broader clinical context.
Conclusions/Impact on practice statement
Inflammation is now recognised as a central contributor to coronary artery disease, influencing plaque initiation, progression, destabilisation, and recurrent ischaemic risk. Contemporary evidence supports the integration of inflammatory biomarkers, advanced imaging, and cardiometabolic profiling into more individualised cardiovascular risk assessment. Anti-inflammatory therapies, particularly colchicine and cytokine-targeted approaches, represent promising adjunctive strategies in selected patients, although uncertainties regarding long-term safety and optimal patient selection remain. Further progress in precision cardiovascular medicine will likely depend on integrated use of biomarkers, imaging, omics technologies, and artificial intelligence-assisted risk stratification to improve prevention and therapeutic decision-making.
