Keywords
Cardiotoxicity; cocaine; heart failure
Take-home messages
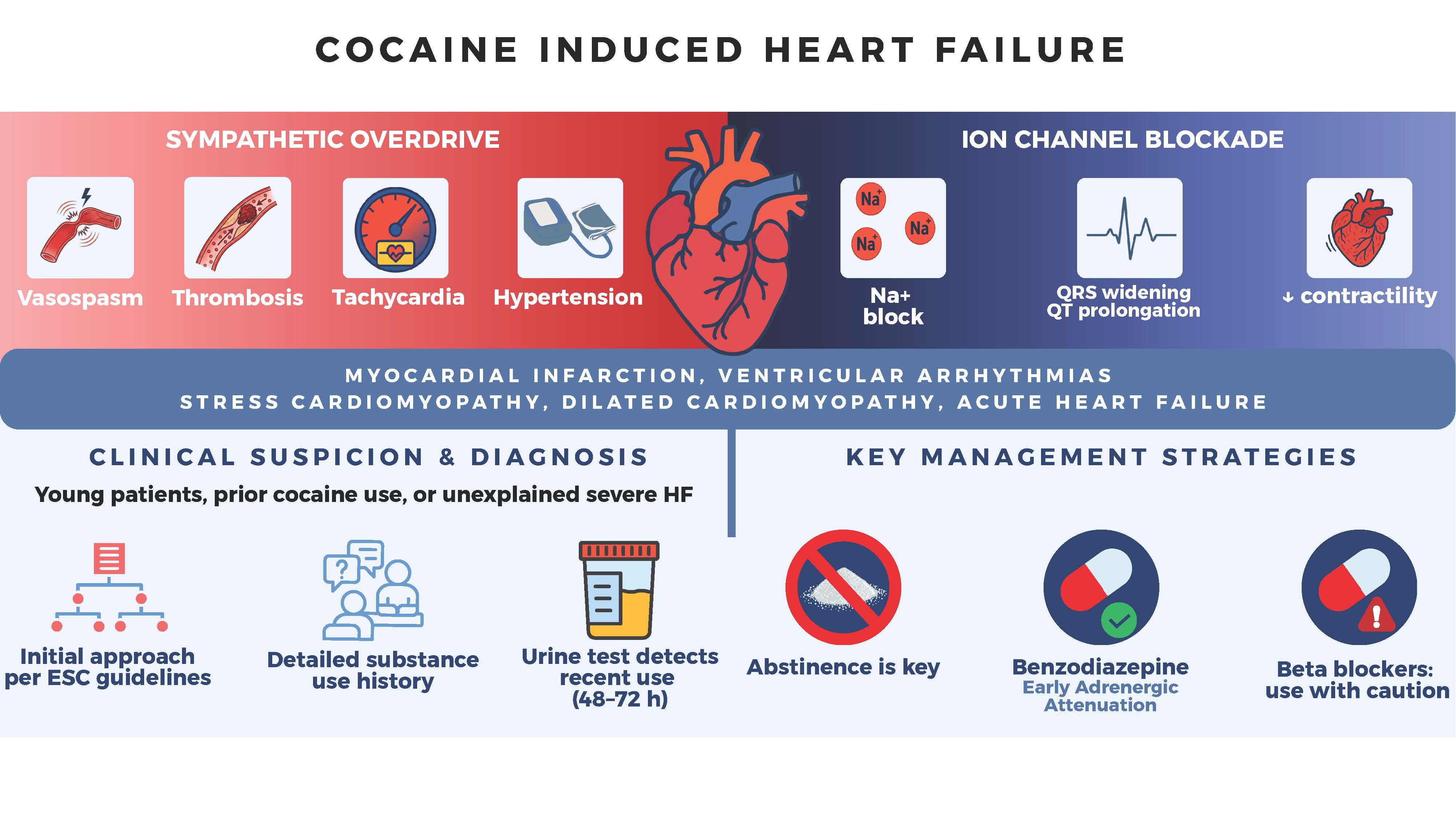
- Cocaine injures the heart via sympathetic overdrive and ion channel blockade. Cocaethylene, formed with alcohol, is even more cardiotoxic and prolongs exposure.
- Urine toxicology is the standard method to confirm recent cocaine exposure. It detects the metabolite benzoylecgonine, which is usually positive up to 48-72 hours after use (longer with heavy or chronic intake). False negatives are possible if testing is delayed; always interpret results with the clinical context.
- Cocaine use is frequently underreported by patients.
- Consider cocaine-related heart disease in patients with prior cocaine use after common causes are excluded.
- Early administration of benzodiazepines is recommended to attenuate adrenergic activation.
- Beta blocker therapy must be used with caution.
Introduction
Cocaine is one of the most commonly used illicit stimulants worldwide, with increasing global production and consumption [1]. Beyond its well-known association with acute coronary syndromes and arrhythmias, chronic cocaine use is an underrecognised cause of heart failure (HF). A systematic review and meta-analysis has confirmed a significant association between chronic cocaine use, structural cardiac abnormalities, and heart failure [2]. Cocaine can induce both acute and chronic myocardial injury through sympathetic overstimulation, coronary vasospasm, prothrombotic effects, and direct myocardial toxicity [3]. Repeated exposure promotes myocardial ischaemia, myocarditis, fibrosis, and progressive left ventricular (LV) dysfunction [4]. For clinicians, recognising cocaine as a potential underlying factor in unexplained cardiomyopathy – especially in younger adults – is crucial, since cardiac function may improve after cessation. Recovery of left ventricular function has been reported after sustained abstinence, although improvement is variable and appears to depend on the duration of exposure and degree of structural myocardial damage [2].
Central illustration. Cocaine-induced heart failure.
How cocaine stresses the heart
Cocaine acts through two complementary toxic pathways that put the myocardium under extreme stress: it injures the heart via a powerful sympathetic surge and direct ion channel blockade [4]. By inhibiting norepinephrine reuptake, it creates a catecholamine storm that leads to tachycardia, hypertension, coronary vasospasm, and a prothrombotic state, sharply increasing myocardial oxygen demand while reducing supply [3]. At the same time, cocaine blocks cardiac sodium channels, slowing conduction and widening the QRS, while its effects on potassium and calcium channels prolong the QT interval and destabilise repolarisation. Together, these complementary mechanisms explain why patients can present with chest pain, acute coronary syndromes, malignant arrhythmias, or even pump failure only minutes after consumption, even in the absence of structural coronary disease.
Table 1. Pharmacological mechanisms of cocaine and clinical consequences. [4,5]
|
Mechanism
|
Clinical/ECG feature
|
Consequence for the heart
|
|
Sympathetic surge (norepinephrine reuptake inhibition)
|
Tachycardia, hypertension, chest pain, ST changes
|
↑ O₂ demand, myocardial ischaemia, infarction
|
|
Coronary vasospasm / prothrombotic state
|
Angina, acute coronary syndrome, elevated troponin
|
Ischaemia, infarction, scarring
|
|
Na⁺ channel blockade
|
QRS widening, conduction delay, wide complex tachycardia
|
Arrhythmias,
↓ contractility,
acute pump failure
|
|
K⁺/Ca²⁺ channel effects
|
QT prolongation, torsades de pointes, ventricular arrhythmias
|
Sudden cardiac death
|
|
Chronic toxicity (inflammation, oxidative stress, fibrosis)
|
Progressive LV dysfunction, dilated cardiomyopathy
|
Chronic HF, sometimes reversible with abstinence
|
|
Alcohol co-use (cocaethylene)
|
Prolonged intoxication, higher arrhythmic burden
|
Enhanced cardiotoxicity,
↑ mortality risk
|
ECG: electrocardiogram; HF: heart failure; LV: left ventricle
Cocaine chronic toxicity: pathways to heart failure
Chronic cocaine use progressively damages the myocardium through a combination of repeated ischaemia, oxidative stress, and direct toxic effects [4]. Episodes of vasospasm and thrombosis produce micro-infarcts and scarring, while inflammatory responses promote myocarditis. Over time, these mechanisms lead to interstitial fibrosis, ventricular remodelling, and systolic dysfunction [2,6]. The typical phenotype is dilated cardiomyopathy, often in relatively young patients without conventional risk factors (except tabagism, often present). Importantly, cardiac function may partially recover after cessation, underlining the importance of recognising cocaine as a reversible cause of HF. However, continued exposure accelerates decline, with an increased risk of arrhythmias, progressive LV dilation and sudden death.
Acute versus chronic heart failure in cocaine users
Cocaine can trigger acute HF even in previously healthy individuals. Mechanisms include severe hypertension from sympathetic surge, malignant arrhythmias (including sudden death) due to ion channel blockade, or acute myocardial depression. Clinically, this may present as sudden death, pulmonary oedema, or cardiogenic shock shortly after use.
In rare cases, the intense catecholamine surge induced by cocaine may precipitate a stress cardiomyopathy (Takotsubo), mimicking acute coronary syndrome but with transient LV dysfunction [7].
With repeated exposure, cocaine promotes structural damage and remodelling, leading to
chronic HF. The typical phenotype is a dilated cardiomyopathy with reduced ejection fraction (EF), although an early diastolic pattern with preserved EF may also occur, especially in hypertensive users. Importantly, LV function may improve after abstinence, underlining the need to identify cocaine as a potentially reversible cause of HF [2].
When to suspect cocaine in heart failure
Cocaine should be considered in any young or middle-aged patient presenting with HF without conventional risk factors. Suspicion is particularly warranted in those with a history of chest pain, palpitations, or arrhythmias following recreational activity. Acute decompensation may occur after binge use, often with intake of other drugs and sometimes with concomitant alcohol intake. Electrocardiographic abnormalities such as QRS widening, QT prolongation or unexplained ventricular arrhythmias should raise concern. A dilated cardiomyopathy of unclear origin, especially if accompanied by recurrent hospitalisations or partial reversibility after periods of abstinence, should prompt enquiry about cocaine use.
Urine toxicology screening remains the standard tool to confirm recent exposure. It detects the metabolite benzoylecgonine, typically up to 48–72 hours after intake, and for longer periods in heavy or chronic users [8]. False negatives are possible if testing is delayed, and results must always be interpreted in the clinical context. Screening is especially useful in unexplained cardiomyopathy, arrhythmias, or acute HF in younger adults. In addition to diagnosis, repeated testing can support counselling and monitoring of abstinence, making it a valuable part of patient management.
In daily practice, clinicians should remember that these combined mechanisms explain why a patient may present with angina, arrhythmia, or acute pump failure within minutes of use, even in the absence of coronary atherosclerosis. Routine history taking is often insufficient, as patients may underreport cocaine use [9].
Epidaemiology
Cocaine use and associated health burden
In 2022, approximately 23.5 million people worldwide used cocaine, representing 0.5% of the population aged 15-64 years. This increase in use has occurred alongside a rise in global cocaine production, which is estimated to have doubled between 2014 and 2020 [1].
In Europe, cocaine use is also increasing markedly and now represents the second most commonly used illicit substance after cannabis. This expansion has been accompanied by a growing burden of related health complications. In 2023, cocaine was mentioned in 25% of cases of acute drug toxicity within the European Drug Emergencies Network’s associated sentinel hospitals, and was implicated in 26% of drug-related deaths across 20 European countries [10].
Cardiovascular consequences of cocaine use
An American study based on National Vital Statistics System data (2014-2023) reported a marked increase in cardiovascular mortality involving psychostimulants (cocaine and amphetamines), with an average annual rise of approximately 10%, in contrast to the relative stability of overall cardiovascular mortality [11]. In a French study based on spontaneous reports submitted by healthcare professionals to the national addiction monitoring network between 2010 and 2016, cardiovascular complications were the third most frequently reported category of adverse effects, after psychiatric and neurological complications [12].
Cocaine use may also adversely affect short-term outcomes following cardiovascular events. In the French prospective multicentre ADDICT-ICCU study, which included 1,499 patients hospitalised in 39 cardiac intensive care units in April 2021, recreational drug use, including cocaine, was associated with a 5.1-fold increase in the risk of major in-hospital adverse events [9].
Cocaine-related heart failure
Although the link between cocaine use and HF is recognised, it has been far less extensively investigated than acute/chronic coronary events. As most evidence is based on isolated case reports or small case series, the true prevalence of cocaine-related cardiomyopathy remains uncertain.
Based on three cross-sectional studies, the prevalence of LV dysfunction among asymptomatic chronic cocaine users may reach up to 5% [2]. Structural cardiac abnormalities are also frequently observed in this population. In one study, including 94 asymptomatic chronic users, cardiovascular magnetic resonance imaging identified cardiovascular abnormalities in the vast majority of participants (71%). Compared to controls, 31% had moderate LV dilatation, 30% had LV hypertrophy, and 13% had concentric remodelling [6].
Among hospitalised patients, the clinical impact appears more pronounced. In a national registry covering 83 hospitals, stimulant use (mainly cocaine) was reported in 5.3% of patients admitted to the emergency department for acute decompensated HF. Compared with non-users, these patients had more recurrent hospitalisations at six months (28% versus 11%) and more severe systolic dysfunction, with a median ejection fraction of 23% versus 40% [13].
Diagnosis
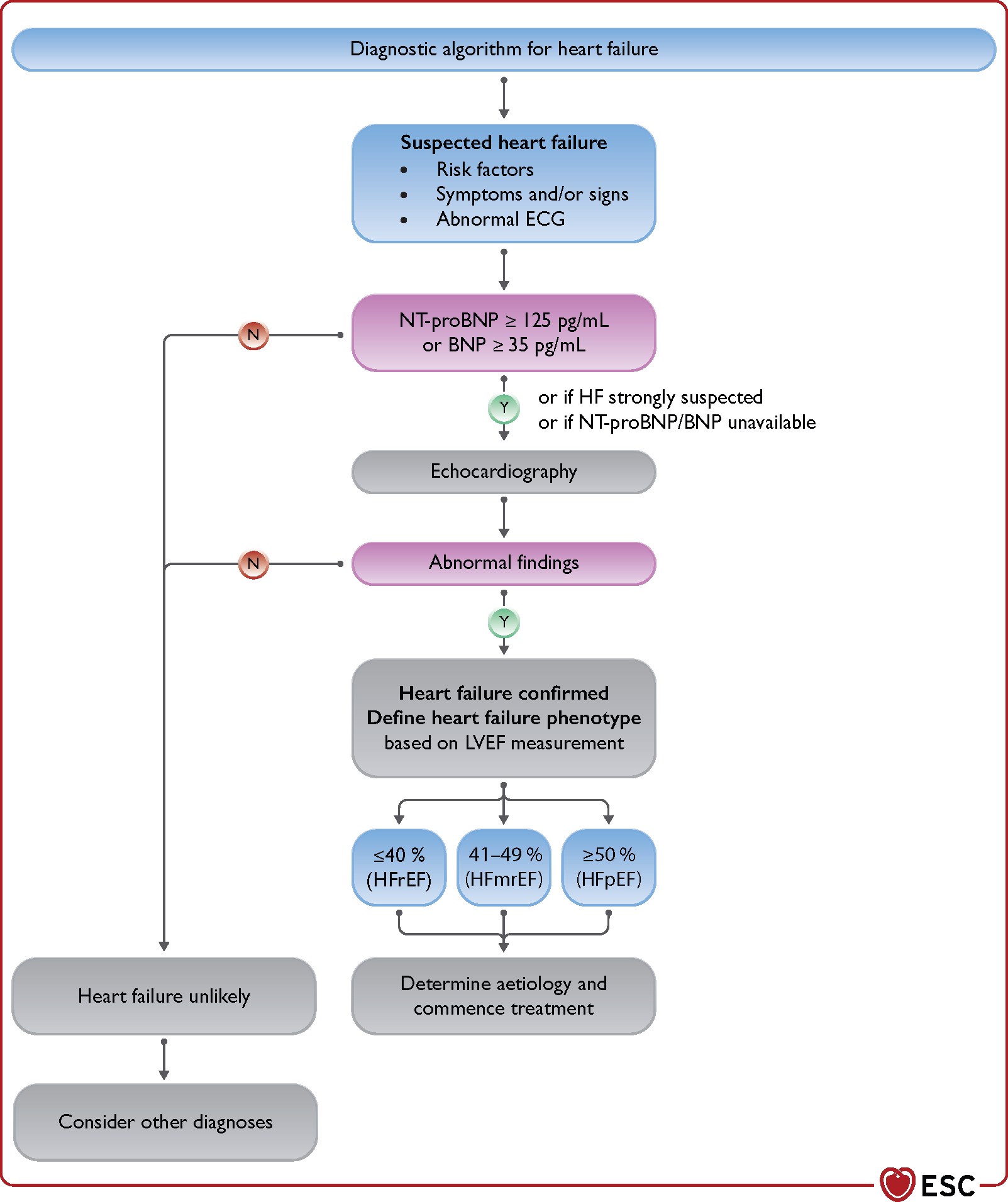
The initial diagnostic approach to cocaine-induced HF is similar to that employed with non-users. According to the 2021 ESC guidelines, the diagnosis is based on the presence of typical symptoms and signs, electrocardiographic abnormalities, elevated natriuretic peptides, and echocardiographic evidence of structural or functional cardiac abnormalities [14] Figure 1.
Figure 1. Heart failure diagnosis.
(Reproduced with permission from [14]).
BNP: B-type natriuretic peptide; ECG: electrocardiogram; HFmrEF: heart failure with mildly reduced ejection fraction; HFpE: heart failure with preserved ejection fraction; HFrEF: heart failure with reduced ejection fraction; LVEF: left ventricular ejection fraction; NT-proBNP: N-terminal pro-B type natriuretic peptide
The possibility of cocaine-related heart disease should be considered in any patient with a documented history of cocaine use, after ruling out the most common causes of HF. In this context, invasive coronary angiography or coronary CT angiography can exclude significant coronary artery disease. Some patients could present concomitant coronary artery disease, necessitating co-management of cardiac diseases. Cardiac magnetic resonance imaging plays a central role in myocardial tissue characterisation and in the differential, particularly in identifying inflammatory, toxic, or ischaemic aetiologies.
A comprehensive clinical history is essential to characterise cocaine use. It should specify the type of substance, route of administration, timing of the last intake, duration and frequency of use, as well as concomitant tabagism, alcohol intake, and other substance use. Nonetheless, underreporting remains common. In the prospective multicentre ADDICT-ICCU study, only 56.5% of patients with positive toxicology results reported illicit drug use [9], although they had given consent for research and had been specifically questioned on these aspects. Therefore, toxicological screening of urine or blood may be useful when clinical suspicion is high, particularly in young patients, severe HF, or when no alternative cause is identified after the initial evaluation.
Management
Whether presenting with acute or chronic HF, the management of patients using cocaine is broadly similar to that of other patients; however, specific considerations apply.
Cocaine use is frequently associated with excessive alcohol consumption and/or concomitant use of other cardiotoxic substances, including amphetamines. Available data suggest that cocaine-related cardiotoxicity may be at least partially reversible [2]. Management of substance use disorder, ideally within a structured addiction programme, remains the cornerstone: sustained abstinence is a key determinant of recovery of LV function and prevention of HF progression.
The deleterious cardiovascular effects of cocaine are primarily mediated through sympathetic overstimulation. Early administration of benzodiazepines is recommended to attenuate adrenergic activation. In some patients, sedation alone may be sufficient to control symptoms and reduce the risk of acute cardiovascular complications [15].
In patients presenting with acute coronary syndromes, standard management including antithrombotic therapy and an early invasive strategy should be considered. However, given the increased risk of stent thrombosis in this population, a conservative approach may be appropriate depending on clinical and angiographic findings [16].
Nitrates and non-dihydropyridine calcium channel blockers (e.g., diltiazem, verapamil) are effective in relieving symptoms, particularly in the presence of coronary vasospasm. These agents may be administered intravenously during the acute phase, with dose titration according to haemodynamic response [17].
Beta blockers are generally not recommended in the early management of patients with recent cocaine use, owing to concerns regarding unopposed alpha-adrenergic stimulation, which may promote coronary vasoconstriction, systemic hypertension, and reduced myocardial perfusion. Although early experimental studies raised concerns regarding unopposed alpha-adrenergic stimulation, contemporary clinical data have not consistently confirmed an increased risk [18].
In selected patients, particularly when cocaine exposure is remote and the anticipated clinical benefit is substantial, beta blocker therapy may be considered after careful risk-benefit assessment. In such circumstances, agents with combined alpha- and beta-adrenergic blocking properties (e.g., labetalol or carvedilol) may be preferred [19]. Close clinical and haemodynamic monitoring is then recommended.
In a nutshell, there are mainly two arrhythmic complications that can be threatening. Wide-QRS sinus tachycardia secondary to sodium channel blockade can develop and should be managed with intravenous sodium bicarbonate, as in tricyclic antidepressant toxicity, typically resulting in QRS narrowing. Secondly, in case of ventricular tachycardia or ventricular fibrillation, management follows standard advanced cardiac life support protocols. Beta blockers should be avoided in the acute setting if ongoing cocaine effects are suspected. To date, no specific safety concerns have been consistently reported with amiodarone use in this context.
In chronic HF, treatment is guided by the presence and severity of LV systolic dysfunction and should follow general guideline-directed medical therapy [14]. It combines a sodium-glucose cotransporter 2 (SGLT2) inhibitor, a mineralocorticoid receptor antagonist, and an angiotensin-converting enzyme inhibitor or angiotensin receptor blocker, with consideration of neprilysin inhibition. The use of beta-blockers in patients at high risk of recurrent cocaine use remains controversial [20]. While earlier concerns suggested potential harm, more recent observational data do not indicate a clear increase in adverse events [2]. Beta blocker therapy may therefore be considered when the expected prognostic benefit is substantial (e.g., with LV systolic dysfunction or ventricular arrhythmias) and the likelihood of recurrent cocaine exposure is low.
Conclusion
Cocaine exposure places the myocardium under dual stress through intense adrenergic activation and ion channel blockade, explaining the broad clinical spectrum from chest pain and arrhythmias to acute pump failure and chronic dilated cardiomyopathy.
What clinicians should know
- Systematically ask about cocaine in young or middle-aged patients with unexplained cardiomyopathy, arrhythmias, or acute decompensated heart failure, and confirm suspicion with urine toxicology when appropriate.
- Recognise that cocaine cardiotoxicity spans acute (hypertensive crisis, acute coronary syndrome, stress cardiomyopathy, malignant arrhythmias) and chronic (dilated cardiomyopathy, diastolic dysfunction) presentations, often without significant coronary atherosclerosis.
- Remember that cardiac dysfunction may improve after sustained abstinence; identify and treat substance use disorder early, ideally within a structured addiction programme, as part of comprehensive heart failure care.
- In the acute phase, prioritise benzodiazepines to blunt adrenergic surge and use nitrates and non-dihydropyridine calcium channel blockers for vasospasm; avoid early beta-blockade when recent cocaine use is suspected.
- For chronic heart failure, apply standard guideline-directed medical therapy (angiotensin-converting enzyme inhibitor, angiotensin II receptor blocker, angiotensin receptor/neprilysin inhibitor, magnetic resonance angiography, SGLT2 inhibitor, and when appropriate, beta blockers), while individualising beta blocker initiation and favouring agents with combined alpha-beta blockade (e.g., carvedilol) when recurrent use is unlikely but arrhythmic or systolic indications are strong.
- Anticipate higher risks of rehospitalisation and adverse in-hospital events in cocaine users with heart failure, and organise close multidisciplinary follow-up involving cardiology, addiction medicine, and, when necessary, psychiatry and social support services. See the ongoing ClinicalTrials.gov: NCT00872599
Open questions/gaps
- Which clinical, imaging, or biomarker profiles best predict reversibility of cocaine-induced cardiomyopathy and long-term outcomes after abstinence? [1,3]
- What is the optimal beta blocker strategy (timing, agent, dosing) in patients with ongoing or intermittent cocaine use and established HF with reduced ejection fraction or ventricular arrhythmias [1,4]?
- How should we refine risk stratification for sudden cardiac death in cocaine-associated cardiomyopathy, including indications for implantable cardioverter-defibrillators in the context of potentially reversible toxicity?
- To what extent do adulterants and co-exposures (such as alcohol leading to cocaethylene) modulate cardiotoxicity and heart failure trajectory, and can specific preventive or therapeutic interventions be defined for these patterns?
Ongoing and recent studies
Several ongoing or recent studies registered on ClinicalTrials.gov and related platforms illustrate current research priorities around cocaine, cardiovascular complications, and heart failure-related populations:
- Addiction in intensive cardiac care (ClinicalTrials.gov: NCT05063097) is characterising the prevalence and impact of recreational drug use, including cocaine, among patients admitted to intensive cardiac care units for acute cardiovascular events and heart failure, building on prior observational cohorts such as ADDICT-ICCU [9].
- Observational studies in acute coronary syndromes with cocaine exposure (e.g., ClinicalTrials.gov: NCT06177860) are delineating clinical and angiographic profiles and short-term complications, mainly in case of acute coronary events, with implications for HF risk and secondary prevention [9].
- Trials of pharmacological strategies for cocaine use disorder and its cardiovascular safety (e.g., pramipexole, doxazosin-modafinil combinations, amantadine-propranolol) are assessing haemodynamic and ECG responses to controlled cocaine administration, which may inform safer cardiovascular management in this population (for instance, pramipexole: ClinicalTrials.gov: NCT01651377; doxazosin and modafinil, alone and in combination: ClinicalTrials.gov: NCT02538744; amantadine: ClinicalTrials.gov: NCT00128349).
- Collectively, these efforts should help refine risk stratification, clarify the role of beta blockers and other HF therapies in chronic cocaine users, and integrate addiction medicine more tightly into the care pathways of patients with cocaine-related heart failure.