

















Keywords
arrhythmia; cannabis; cardiomyopathy; heart failure; myocardial infarction; stroke; vascular inflammation
Take-home messages
- Cannabis use is on the rise due to changes in regulation worldwide.
- Modern cannabis products are more potent with new delivery systems.
- Cannabis is linked to heart disease, including myocardial infarction, arrhythmia, stroke, and heart failure.
- Cannabis use is associated with drug interactions.
- Clinicians should consider screening for cannabis use as a modifiable risk factor.
Introduction
Cannabis is a commonly used psychoactive drug [1], composed of hundreds of chemical components called cannabinoids. The most abundant cannabinoids are delta-9-tetrahydrocannabinol (THC) and cannabidiol (CBD), of which THC produces more psychoactive effects. Cannabis has been used by humans for centuries for recreational and medicinal purposes. At the beginning of the 20th century, a prohibition movement in the United States sought to restrict cannabis use, which was ultimately deemed high-risk and classified as a Schedule 1 drug. Other countries around the world also imposed strict regulations on cannabis use. To this day, several former member states of the Soviet Union and China, amongst others, prohibit cannabis use.
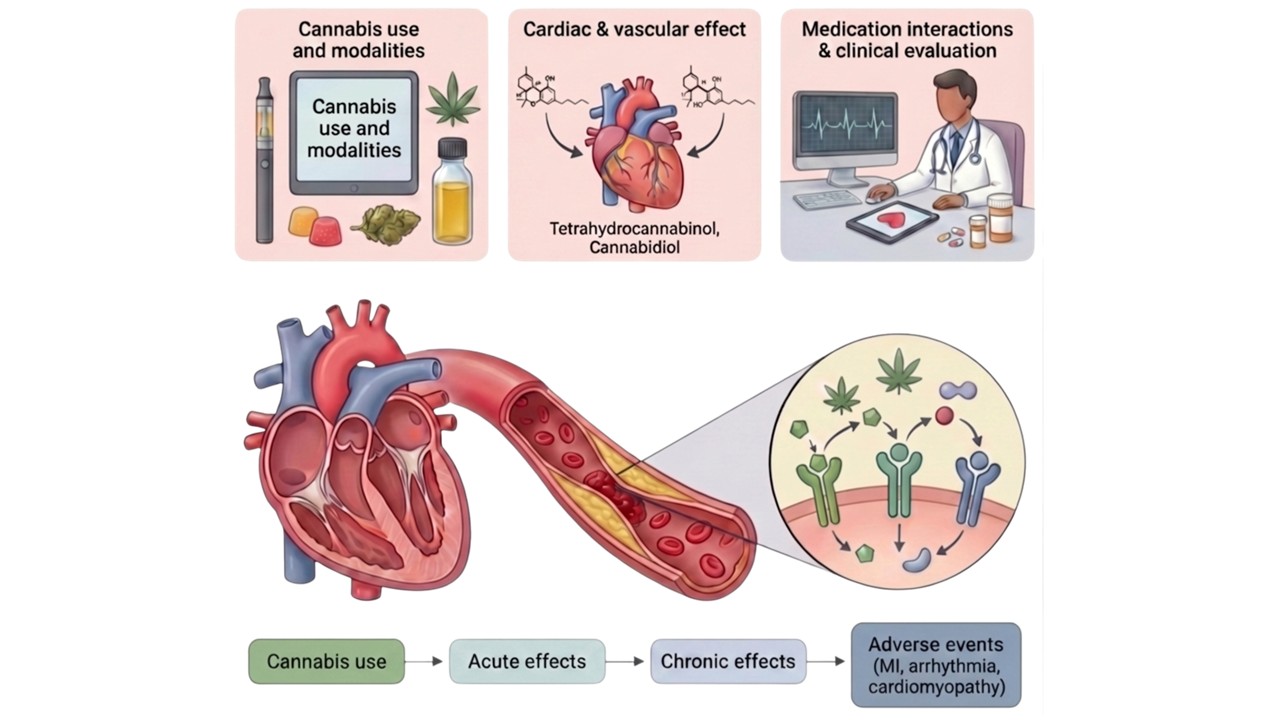
Central illustration. Cannabis use is on the rise with new modalities of consumption.
The cardiovascular effects of 9-tetrahydrocannabinol (THC) and cannabidiol (CBD) are emerging. Cannabis interacts with cardiac medications and may cause adverse events. The acute and chronic effects of cannabis are linked to myocardial infarction (MI), arrhythmias, and cardiomyopathy. (Generated with Illustrae.co. and BioRender)
Over the past few decades, growing societal acceptance of cannabis has led to a shift in its regulation, increasing its accessibility for medical and recreational use (Figure 1). In the past, modes of cannabis consumption were limited to “joints” or cigarettes, but due to the commercialisation of the drug, it can now be consumed in many other forms such as vaping, “edibles,” beverages, and topical oils [2]. Cannabis is also increasingly consumed by the elderly, who are at high risk for cardiovascular events.
Figure 1. The legal status of cannabis around the world. (Reproduced with permission from Nature Review Cardiology [1])
The regulation of cannabis varies considerably worldwide and is changing rapidly, along with perceptions of the safety and usage of the drug.
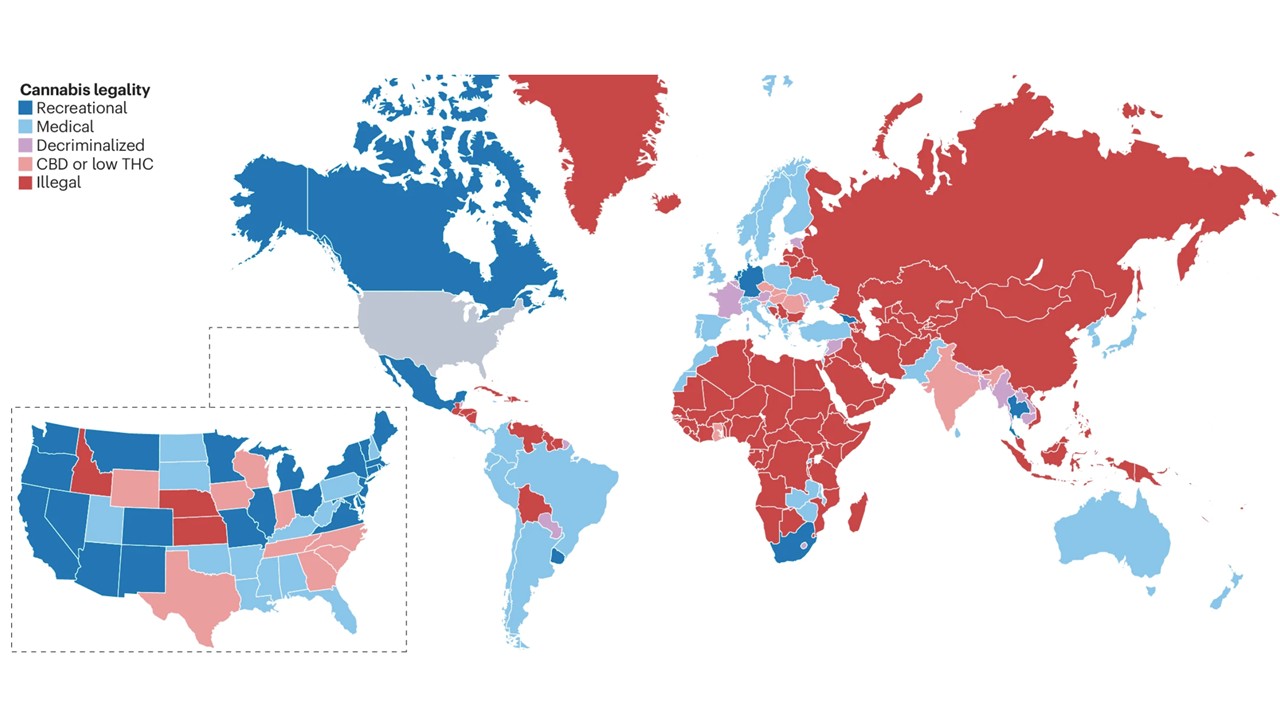
CBD: cannabidiol; THC: tetrahydrocannabinol.
Due to longstanding research restrictions, many in the public perceive cannabis as benign or even beneficial, with some believing it to be a panacea for ailments. With respect to the heart, an early study suggested that low-dose, oral cannabis might be protective for the heart [3]. More recently, emerging clinical data and physiologically relevant preclinical models found that THC is linked to vascular dysfunction and atherosclerosis [4,5]. The relationship between cannabis and cardiovascular disease is complex and depends on the route of administration, dose, types of cannabinoids, and co-use with tobacco. Moreover, epidemiological studies suggest that cannabis can exacerbate cardiovascular events, arrhythmias, and heart failure. The goal of this article is to provide a concise, up-to-date overview of the evidence of the potential risks of cannabis use for the general cardiologist.
Cannabis and the endocannabinoid system
The endocannabinoid system is important for mood, memory, satiety, and learning. The endocannabinoid system comprises traditional cannabinoid receptors, including cannabinoid receptor 1 (CB1) and cannabinoid receptor 2 (CB2). CB1 is expressed throughout the central nervous system and peripheral tissue as well as in the vasculature (Figure 2). Stimulation of the CB1 pathway promotes atherosclerosis by increasing sympathetic tone, endothelial dysfunction, and modulating vascular tone. CB2 receptors are expressed in immune cells and exert anti-inflammatory effects, leading to vascular quiescence.
Figure 2. Mechanism of action of cannabinoids on cardiovascular health. (Reproduced with permission from Nature Review Cardiology [1])

When Δ9-tetrahydrocannabinol (Δ9-THC) binds to cannabinoid receptor 1 (CB1), the G protein-coupled receptor (GPCR) is activated, and the Gi/o complex dissociates into the Giα, βγ, and β-arrestin subunits, which regulate heart rate, blood pressure, hypertension, atherosclerosis, and cardiomyopathy. The Giα subunit inhibits adenylate cyclase, blocking cAMP production and preventing phosphorylation of protein kinase A and its downstream effects on transcription. β-Arrestin modulates extracellular signal-regulated kinase 1 and 2 (ERK1/2; also known as MAPK3 and MAPK1, respectively) and c-JUN amino-terminal kinase (JNK) pathways. The βγ subunit activates the mitogen-activated protein kinase (MAPK) pathway, promotes the nuclear translocation of nuclear factor-κB (NF-κB), activates transcription of genes encoding pro-inflammatory factors, and suppresses transcription of genes encoding factors that protect against oxidative stress. Therefore, CB1 agonists promote endothelial dysfunction and atherosclerosis. Cannabinoid receptor 2 (CB2) agonists, such as JW133, activate the GPCR, leading to dissociation of the subunits. The βγ subunit activates the MAPK–p38 pathway but prevents translocation of NF-κB to the nucleus. Consequently, the transcription of pro-inflammatory genes is not activated, and the transcriptional status of oxidative stress-protective genes is not perturbed. CB2 agonism causes endothelial cells to produce nitric oxide (NO) and other vasoactive substances that modulate blood pressure. β-Arrestin promotes nitric oxide synthase 3 (NOS3) production and, consequently, NO release, leading to vascular quiescence. The binding of agonists to CB1 and CB2 also modulates various channels, including transient receptor potential cation channel subfamily V member 1 (TRPV1), voltage-gated calcium channel (VGCC), G protein-coupled inwardly rectifying potassium channel (GIRK), and sodium and potassium channels, activating the inositol trisphosphate (IP3) pathway that causes calcium release, protein phosphorylation and activation of calcium-binding proteins. ROS, reactive oxygen species.
Phytocannabinoids cause their effect via the endocannabinoid system. Cannabis is composed of hundreds of cannabinoids, with the most abundant and well-studied being THC and CBD. The effects of other cannabinoids on the cardiovascular system are largely unknown. Next-generation synthetic cannabinoids, such as “Spice” and “K2”, have a strong binding affinity for CB1 and may produce a zombie-like state, which could damage the cardiovascular system and merit further investigation [6].
Routes of administration
Cannabis is consumed using multiple routes and modalities [2,7]. Traditionally, cannabis was consumed in joint or cigarette form, producing particulate matter, carbon monoxide, and other toxins. With the development of e-cigarettes, cannabis can now be vaped. While vaping avoids combustion, it heats components in combination with atmospheric contaminants, which produces hazardous and potentially hazardous compounds for the cardiovascular system.
Oral ingestion of cannabis has expanded in response to changing regulations and commercialisation. Cannabinoids can be consumed orally in a variety of forms, including candies, gummies, and other foods. In addition, cannabinoids can be consumed as beverages. Cannabinoids are lipid-soluble and can also be applied topically as creams or lotions and absorbed through the skin.
Inhalation and vaping produce the highest concentration of, and peak exposure to, cannabinoids, heightening the risk of arrhythmias and cardiovascular disease. Oral ingestion is limited by absorption and first-pass hepatic metabolism, which restrict the maximum concentration of cannabinoids in the body. However, delayed overconsumption can lead to intoxication and misadventure. Moreover, heavy cannabis use can lead to psychological disorders such as cannabis use disorder, anxiety, or psychotic disorders [7].
Potential beneficial effects
Cannabis is perceived by many as benign, and early research suggested an anti-inflammatory effect in cardiovascular disease [3]. Cannabis also has been used for centuries for analgesia and sedation [1]. In paediatrics, there appears to be compelling evidence for using cannabidiol (Epidiolex) in treating seizure disorders such as Dravet's or Lennox-Gastaut syndrome [8,9]. The U.S. Food and Drug Administration approved a synthetic THC, dronedarone, for medicinal use to relieve nausea caused by chemotherapy in cancer patients. A meta-analysis revealed that cannabis has a small but significant benefit for nausea and vomiting [10]. Cannabis has also been used in the setting of HIV cachexia to promote appetite, and a meta-analysis found a moderate effect on increasing body weight [10]. Cannabis is touted as an alternative to opioids for analgesia for chronic pain and sedation, yet evidence from randomised clinical trials thus far does not support this claim [10].
Cardiovascular risk factors
The effects of cannabis on cardiovascular risk factors are complex [1]. Cannabis use is associated with an increased body mass index, but there is conflicting evidence about its effect on insulin resistance and diabetes. Cannabis use is also reported to have no effect on lipid levels. The haemodynamic effects of cannabis have been studied extensively in multiple animal and clinical studies, which have found that it produces both acute and chronic effects on haemodynamics. Upon ingestion, cannabis acutely increases sympathetic tone and causes tachycardia and hypertension and is subsequently followed by bradycardia and hypotension [11]. While some studies have linked cannabis with hypertension, numerous animal and clinical studies show that chronic cannabis use is associated with hypotension. The combined effect, or co-use, of cannabis and tobacco is unclear, but because tobacco allows for deeper inhalation and causes adverse cardiovascular effects via distinct mechanisms, it is likely that co-use will cause synergistic adverse effects on the cardiovascular system and the body in general [7].
Links to cardiovascular disease
Cannabis use was difficult to study in the past because it was a Schedule 1 drug in the US, and legal access to it was largely restricted internationally. The proposed mechanisms for cannabis-mediated cardiovascular disease include haemodynamic stresses, coronary vasospasm, endothelial dysfunction, platelet activation and thrombosis. Prior to regulatory changes, data on cannabis-mediated cardiovascular disease were limited to case reports or case series of young adults with heavy cannabis use presenting with myocardial infarction (MI). Angiograms revealed normal coronaries or minimally obstructive coronary artery disease, and events were attributed to vasospasms. Epidemiological data now suggest that cannabis use is linked to atherosclerotic cardiovascular disease and death [2,7,12,13], which have since been corroborated with compelling links between cannabis use and cardiovascular disease [2,12,14,15]. Independent of the route of administration, heavier cannabis use is associated with adverse cardiovascular events in a dose-dependent manner [5,16]. In a cross-sectional study, daily cannabis use was associated with a 16% increase in coronary heart disease, a 25% increase in MI, and a 42% increase in cerebrovascular accident (CVA) [16,9]. A study from the UK Biobank found that cannabis use is associated with increased cardiovascular events and death in women [17]. There is also emerging evidence that cannabis use is linked to a threefold increase in peripheral vascular disease [18]. A recent meta-analysis revealed that cannabis use has an estimated risk ratio of 1.29 (95% confidence interval [CI]: 1.05-1.59) for acute coronary syndrome, 1.20 (95% CI: 1.13-1.26) for CVA, and 2.10 (95% CI: 1.29-3.42) for cardiovascular death [19].
Arrythmias
Cannabis is associated with tachyarrhythmias, including supraventricular and ventricular arrhythmias, and bradyarrhythmias. The mechanisms may include catecholaminergic surge, autonomic instability, MI, and perturbation of ion channels. The DANISH study prospectively followed patients on oral medical cannabis for chronic pain. After just 180 days, the study found a twofold increase in new onset arrhythmias (0.8% vs 0.4%) [20], which are mostly supraventricular arrhythmias such as atrial fibrillation. The increased signal for CVA from cannabis might be due to atherosclerosis or atrial fibrillation.
Heart failure and cardiomyopathy
Cannabis can cause myocarditis [1,21]. Evidence suggests that cannabis causes heart failure [22]. However, the increased incidence of heart failure is attributed to a rise in acute coronary syndrome, leading to ischaemic heart disease. Moreover, the haemodynamic shifts caused by cannabis use are likely to impair cardiac function and lead to further exacerbation of heart failure.
Drug interactions
Cannabis is an inhibitor of P450, which impairs hepatic metabolism and increases drug exposure [23]. CBD is a potent inhibitor of P450, and THC can affect P450 with chronic use. Therefore, cannabis can interact with cardiovascular medications. Cannabis impairs CYP2C9 and can increase the blood concentration of warfarin, which could increase the international normalised ratio and bleeding risk. CYP3A4 is also impaired with cannabis use and affects the metabolism of statins, thus increasing the risk of myopathy and rhabdomyolysis. Antiarrhythmics such as amiodarone are metabolised via P450 genes. Increased concentrations of antiarrhythmics could lead to QT prolongation and proarrhythmic risk, which could be exacerbated by the sympathetic activation associated with the haemodynamic effects of acute cannabis exposure. Lastly, cannabis can perturb P2Y12 inhibitors such as clopidogrel, by reducing activation, thus rendering recently revascularised patients susceptible to in-stent thrombosis.
Impact on clinical practice
Similar to the emergence of tobacco in the 20th century, cannabis is poised to make a significant impact on cardiovascular health in the 21st century. Tobacco use initially was perceived by many as benign or even healthy, propelling mass consumption and exposure. After decades, when tobacco use was finally linked to lung disease, cancer, and heart disease, healthcare policies and regulations were put in place to limit its harms. With a similar trajectory to tobacco use, cannabis use may exert similar adverse effects on heart health by increasing the rates of MI and arrhythmias, and ultimately lead to heart failure. Clinicians should consider screening for cannabis use not only as a potential modifiable risk factor, but as a drug that could interfere with the safe dosing of concurrent medications used by patients. Aside from the current repertoire of medical and interventional therapies for heart disease, there are no clinically validated treatments to prevent or mitigate the consequences of cannabis-mediated heart disease. As with smoking, the overall best advice that we can give cannabis users is to avoid using it, because quitting is better than the purported therapeutic benefits of the drug.

