















Key words
cardiovascular disease; hypertension; pregnancy complications; women
Abbreviation list
CVD: cardiovascular disease
ESC: European Society of Cardiology
LDL: low-density lipoprotein
HDL: high-density lipoprotein
Take-home messages
- Assessment of CVD risk is more complicated in women than it is in men.
- Many traditional CVD risk factors, including hypertension, which accounts for one-third of cases in women, have a stronger relative influence on CVD in women than men.
- Women with a history of hypertensive pregnancy complications need lifelong annual blood pressure measurements for early detection of hypertension.
- Non-traditional CVD risk factors are often underrecognised in women.
Introduction
Differences between women and men have been described in the vast majority of literature on cardiovascular diseases (CVD), including in relation to epidemiology, pathophysiology, risk factors, clinical manifestations, disease progression, and the effects of therapy [1]. Both biological sex (sex chromosomes, sex hormones, and reproductive events) and sociocultural gender (lifestyle, nutrition, smoking, exercise, perceived stress) independently impact cardiovascular health, but more often interact jointly to affect CVD [2]. Typically, biological sex may influence disease pathophysiology and response to treatment, while gender may influence patient behaviour and interaction with the health care system, further influencing treatment options and therapeutic response [2]. While CVD research has traditionally been male-oriented, increasing research and knowledge about CVD in women has emerged over the past decade thanks to dedicated public and private funding of research on CVD in women. Still, women remain one of four societal groups identified by the Lancet Regional Health Europe Commission in 2024 who are impacted by challenges and disparities in cardiovascular health [3]. In particular, among patients with ischaemic heart disease, mortality rates are increasing in women while declining overall [4]. However, while deaths due to ischaemic heart disease are declining in western societies, deaths due to other CVD are increasing, particularly deaths from hypertensive heart disease and heart failure [5]. In Norway, 23% of deaths were caused by CVD in 2024, and more women than men died from hypertension and heart failure.
Sex- and gender-informed medicine may improve CVD prevention in general, including better identification of women at high risk of CVD. In this paper we highlight how CVD risk in women may be better assessed based on recent recommendations [6].
Assessment of CVD risk in women
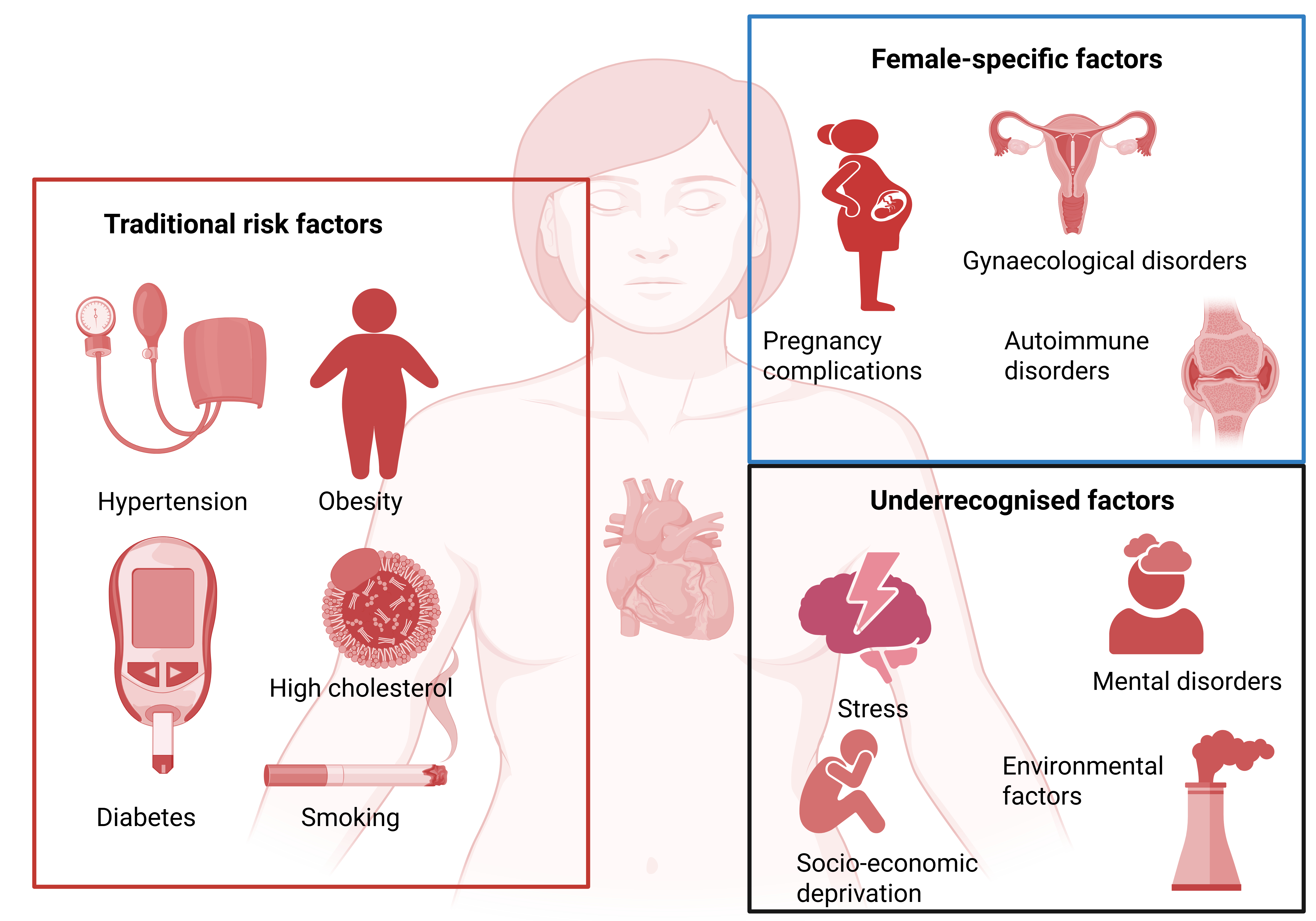
The Lancet Women and Cardiovascular Disease Commission has provided a framework for CVD risk assessment in women, grouping CVD risk factors into traditional, female-specific, and underrecognised CVD risk factors [7] (Figure 1). This framework was used in a recent analysis of population attributable risk for incident heart failure among women in a study using data from the UK Biobank [8]. Less than half of women who developed heart failure were identified when only traditional risk factors were assessed. Thus, assessment using a broader range of CVD risk factors is advised in women.
Central illustration. Key traditional, female-specific, and underrecognised cardiovascular risk factors in women. Created in BioRender. Gerdts, E. (2026) https://BioRender.com/bnia60a.
Traditional CVD risk factors
Hypertension, smoking, obesity, and diabetes mellitus are traditional CVD risk factors, all of which affect CVD risk more strongly in women than in men [9]. Hypertension is the leading risk factor for CVD in women, accounting for approximately one-third of cases [10]. Blood pressure is considered an attributable risk of CVD at a lower blood pressure level in women than in men, the risk being already evident from a blood pressure level of 130/80 mmHg [11]. Furthermore, hypertension often clusters with other traditional CVD risk factors [12]. In women, concomitant obesity and renal dysfunction (reduced estimated glomerular filtration rate) are particularly prevalent. When hypertension is present, women are more susceptible to develop cardiac organ damage, even during antihypertensive treatment [13]. Obesity is a particularly strong risk factor for heart failure with preserved ejection fraction in women [9] and triples the risk of hypertension and cardiac organ damage such as left ventricular hypertrophy. Dietary habits and a sedentary lifestyle may promote obesity.
Elevated cholesterol is also a major contributor to CVD in women. Atherosclerosis is caused by progressive deposition of low-density lipoprotein (LDL) cholesterol and other apolipoprotein B-containing lipoproteins within the arterial walls. Lipid levels vary throughout the menstrual cycle and are highest during ovulation. During pregnancy, LDL cholesterol increases by about 30% and triglycerides by around 50%. LDL cholesterol also increases following oestrogen decline after menopause. Thus, serum LDL cholesterol, total serum cholesterol, and non-high-density lipoprotein (HDL) cholesterol values are all higher in women than men from age 55 onwards [14]. This LDL-cholesterol increase is not benign, as an increase of 1 mmol/L has the same effect on the increase of CVD risk in both women and men.
The European Society of Cardiology (ESC) recommend the Systematic Coronary Risk Evaluation 2 (SCORE2) and SCORE2-Older Persons (SCORE2-OP) for the calculation of the 10-year risk of combined CVD death, non-fatal myocardial infarction and stroke in women and men. Age- and sex-specific risk estimates are based on three traditional CVD risk factors (systolic blood pressure, non-HDL cholesterol, and smoking) and calibrated to different European risk regions. It is well accepted that SCORE2 may underestimate CVD risk in many women. To compensate for this, the 2024 ESC guidelines on hypertension management suggested using a broader spectrum of risk factors, including selected female-specific and underrecognised factors, and a broader screening for cardiovascular organ damage in individuals with blood pressure approaching the treatment threshold (130-139/80-89 mmHg) [6].
Female-specific CVD risk factors
A number of factors associated with fertility, pregnancy, and gynaecological disorders are associated with increased CVD risk (Figure 1). Women with a history of hypertensive disorders of pregnancy, including gestational hypertension and pre-eclampsia, have a twofold higher risk of CVD even before menopause when compared with women without these pregnancy complications. Women with a history of pre-eclampsia develop a chronic cardiovascular inflammation which predisposes them to atherosclerosis, which may be diagnosed by computed tomography coronary artery calcium score in midlife [15]. These women also have a threefold higher risk of dementia later in life [15]. Gestational diabetes is associated with a twofold increase in CVD risk. Preterm delivery, more than three recurrent miscarriages, and one or more stillbirths are associated with a 40% relative increase in CVD risk. The 2024 ESC guidelines on management of hypertension consider these pregnancy complications to be CVD risk modifiers, i.e., the presence of any of these will upgrade a moderate (5 to <10%) 10-year SCORE2 to high (≥10%) CVD risk. The clinical relevance is particularly present in women with persistently elevated blood pressure (130-139/80-89 mmHg), i.e., one close to the treatment threshold.
Many women experience a transition from low to high CVD risk during the perimenopausal period. The premenopausal cardioprotective effects in women may in part result from oestrogen-associated renin-angiotensin-aldosterone system (RAAS) inhibition [12]. The decline in circulating oestrogen and progesterone leads to the activation of RAAS and the sympathetic nervous system, reduced nitric oxide production in the endothelium, and increased sodium and water retention. About 30% of women develop hypertension within a year after menopause, which represents nearly half of women who develop hypertension over the course of their lifetime. Early menopause (<40 years) is associated with increased CVD risk. In a nationwide Danish registry study on endometriosis, a gynaecological disorder where endometrial-like tissue is present at extra-uterine locations causing chronic inflammation, was associated with an 11% higher risk of heart failure over 40 years of observation, independent of traditional cardiovascular risk factors [16]. Up to 16% of women are affected by polycystic ovary syndrome [15]. These women have an increased risk of hypertension, diabetes, dyslipidaemia, and hypertensive pregnancy complications.
Underrecognised CVD risk factors
Several underrecognised factors have been documented to increase CVD risk beyond traditional CVD risk factors [6]. In particular, increased CVD risk in women is associated with psychosocial factors such as mental disorders, abuse, partner violence, and socio-economic deprivation; environmental factors, such as air pollution; and other factors, such as South Asian race/ethnicity, a family history of premature onset of atherosclerotic CVD (before the age of 55 years in first-degree male relatives or before the age of 65 years in first-degree female relatives). Although autoimmune disorders are not sex-specific risk factors, women are disproportionately affected by them: 7 out of 10 patients with such disorders are female. Sex biases in the prevalence of autoimmune disorders are well demonstrated, with rheumatoid arthritis and systemic lupus erythematosus being more prevalent in women, while moderate-severe psoriasis is equally prevalent in both sexes. The presence of these autoimmune disorders has been associated with at least a 40% higher CVD risk. The 2024 ESC Guidelines for the Management of Elevated Blood Pressure and Hypertension consider the presence of these factors to be risk modifiers, i.e., in individuals with these factors and a 10-year SCORE2 risk of 5 to <10%, risk should be upgraded to high (≥10%) [6]. Finally, women are particularly vulnerable to chronic stress, which increases CVD risk via brain-heart crosstalk, involving the activation of the amygdala by means of the central autonomic network, which increases the activation of the sympathetic nervous system and the hypothalamic-pituitary-adrenal axis, leading to catecholamine release, myelopoiesis activation, and the release of pro-inflammatory cytokines with deleterious cardiovascular effects [17].
Management of CVD risk in women
While many female-specific risk factors cannot be prevented in women, the risk of pre-eclampsia and polycystic ovary syndrome may be reduced by controlling traditional CVD risk factors such as obesity. The identification of female-specific CVD risk factors should increase the awareness of high CVD risk both in the patient and in the attending healthcare provider and should prompt greater attention to traditional CVD risk factors such as hypertension, obesity, and hypercholesterolaemia. In particular, an annual CVD risk assessment is recommended in women from the age of 40 years. In women with a history of pregnancy complications, as detailed above, an annual measurement of blood pressure is recommended [18].
Management of hypertension in women
Women with confirmed systolic blood pressure of ≥140 mmHg or diastolic blood pressure of ≥90 mmHg have hypertension and should start antihypertensive drug therapy without delay [6]. A single pill combination of an angiotensin receptor blocker or angiotensin converting enzyme inhibitor (ACEi) with a calcium channel blocker (CCB) of the dihydropyridine group, or a hydrochlorothiazide (HCTZ) in low dose is recommended as the first step. The treatment target is a blood pressure of 120-129/70-79 mmHg in most women, provided the treatment is well tolerated. If blood pressure remains above this level after four weeks’ treatment, a switch to a single-pill combination of three drugs is recommended. Because of biological differences, adverse drug effects differ between women and men. Women more often report adverse effects of ACEi (dry cough), CCB (ankle oedema), beta blockers (tiredness, nightmares), and HCTZ (serum electrolyte disturbances). It is important to inform women about the treatment goal and any potential adverse drug effects that may occur in around 10% of patients, and to adjust the drug treatment accordingly. Treatment adherence may be positively influenced by introducing home blood pressure measurements, but clear instructions about when and how to measure blood pressure must be given. We recommend using a validated automatic or semiautomatic device (see list at www.stridebp.org) with an appropriately sized upper arm cuff for the individual patient. Three consecutive measurements should be performed at 1 minute intervals after an initial five-minute rest in a seated position with the cuff attached to the upper arm. Measurements should be made both morning and evening at 12 hour intervals for 3-5 consecutive days. An average home reading ≥135/85 mmHg indicates uncontrolled blood pressure, in which case the drug treatment should be adjusted. The treatment target for home blood pressure is 120-130/70-80 mmHg. Uncontrolled blood pressure is more common in elderly women compared with men of similar age. This may be due to lower compliance, more adverse drug effects, physician inertia, use of suboptimal drug combinations, or established organ damage. Early and personalised treatment is the best strategy to reduce CVD in women.
Management of hypercholesterolaemia in women
In women without known atherosclerotic cardiovascular disease (primary prevention), SCORE2/SCORE2-OP should be used to assess 10-year risk of CVD. In women with high CVD risk and LDL cholesterol ≥2.6 mmol/L despite non-pharmacological measures, lipid lowering drug treatment with a statin is indicated [19]. Most women with hypertension have high CVD risk (a ≥10% 10-year CVD risk according to SCORE2). Similarly, in women with very high 10-year CVD risk and LDL cholesterol ≥1.8 mmol/L despite non-pharmacological measures, lipid lowering drug treatment with a statin is also indicated. Lipid lowering drug treatment is indicated in all women with diabetes or CVD irrespective of LDL cholesterol level (secondary prevention) [19,20].
Conclusion/Impact on practice statement
Optimal CVD risk assessment in women includes the evaluation of traditional, underrecognised, and female-specific risk factors. Many important factors are easily recognised by using relevant medical history. SCORE2 should be used to calculate the 10-year risk of CVD in women without established CVD or hypertension. In women with moderate (5 to <10%) 10-year CVD risk as evaluated by SCORE2 or blood pressure close to the treatment threshold, attention must be given to underrecognised or female-specific risk factors that may upgrade CVD risk to high, thereby identifying women who will benefit from guideline-recommended CVD prevention.

