















Keywords
autoimmune, cancer, infection, pericarditis, treatment
Abbreviations
AMI: acute myocardial infarction
ANA: anti-nuclear agents
CRP: C-reactive protein
ESR: erythrocyte sedimentation rate
ESRD: end-stage renal disease
NSAID: non-steroid anti-inflammatory drugs
PCIS: post-cardiac injury syndromes
SLE: systemic lupus erythematosus
TB: tuberculosis
Patient-oriented messages
What is an idiopathic pericarditis?
The term idiopathic means without a known cause, following exclusion of the most common and treatable conditions (e.g., systemic inflammatory diseases, neoplastic diseases, tuberculosis or other bacterial causes) [1].
What is the treatment of an idiopathic pericarditis?
Aspirin or non-steroid anti-inflammatory drugs (NSAIDs) are the mainstays of therapy for acute pericarditis. Colchicine is usually added as well because it can halve recurrences.
When is pericarditis a serious illness and when is it not?
The majority of idiopathic pericarditis have a self-limiting, benign course with an overall good prognosis. A more inauspicious prognosis is associated with the neoplastic, purulent, tuberculous, post-traumatic, iatrogenic and autoimmune forms.
The most common secondary malignant tumours associated with pericarditis are lung cancer, breast cancer, malignant melanoma, lymphomas and leukaemia.
Impact on Practice statement
Is an idiopathic pericarditis always a benign illness or can there be complications?
Severe complications of idiopathic pericarditis are rare (<1% constrictive pericarditis, <2% pericardial effusion with cardiac tamponade) but 15%-30% of patients with idiopathic acute pericarditis who are not treated with colchicine will develop either recurrent or incessant forms of the disease, while colchicine may halve the recurrence rate. In any case, the long-term prognosis of patients with viral or idiopathic pericarditis is usually good.
Are NSAIDs and colchicine the only therapeutic options for idiopathic pericarditis?
Aspirin or NSAID + colchicine + exercise restriction are the first-line therapies. The second line therapy includes low-dose corticosteroids (in case of contraindications to aspirin/NSAID/colchicine and after exclusion of an infectious cause).
Recurrent and refractory pericarditis may require a therapy such as intravenous immunoglobulins, anakinra or azathioprine, or ultimately, a pericardiectomy.
Are there indications for the follow-up of idiopathic pericarditis?
Patients at low-risk can be managed as outpatients.
An evaluation of the patient’s response to anti-inflammatory therapy is recommended after 1 week (2015 ESC Guidelines recommendation, Class I, Level of Evidence B) [2].
A mild idiopathic effusion (<10 mm) is usually asymptomatic, generally has a good prognosis and does not require further monitoring.
Moderate effusions (>10 mm) are usually evaluated at 6 months. Large effusions (>20 mm) may worsen and may evolve towards cardiac tamponade in up to one-third of cases and the appropriate follow-up is every 3-6 months.
Individually tailored follow-ups are warranted based on the relative stability or evolution of the size of the effusion.
Take-home message
- Diagnostic ‘Tip and Tricks’ of idiopathic pericarditis
- Therapeutic ‘tip and tricks’ for idiopathic pericarditis
- When an acute pericarditis is complicated or is not going to remission
- How to distinguish incessant, recurrent and chronic pericarditis from the secondary forms and the most probable secondary forms
Diagnostic ‘Tip and Tricks’ of idiopathic pericarditis
1) What the Guidelines say:
In case of a first episode of acute pericarditis, the routine diagnostic practice according to the 2015 ESC Guidelines should include a careful patient history, clinical exam, an electrocardiogram (ECG), chest X-ray, echocardiogram, and routine blood samples that should include inflammatory indices (C-reactive proteins [CRP], erythrocyte sedimentation rate [ESR]), troponin and thyroid function tests.
2) Imaging:
A chest X-ray is recommended for all patients with suspected acute pericarditis (ESC Guidelines recommendation Class I, Level of Evidence C). A chest X-ray is generally normal in patients with acute pericarditis since an increased cardiothoracic ratio only occurs with pericardial effusions exceeding 300 ml. In the case of pleuropulmonary diseases, signs of pleuro-pericardial involvement may be found in patients with pericarditis.
A transoesophageal echocardiogram offers no additional information since it views the heart from its posterior surface and the visualisation of the pericardium is reduced.
Computed tomography (CT) or cardiovascular magnetic resonance (CMR) should be considered in suspected cases of loculated pericardial effusion, pericardial thickening and masses, as well as associated chest abnormalities (ESC Guidelines recommendation Class II, Level of Evidence B).
Evidence of pericardial inflammation found through imaging (CT, CMR), may be an additional diagnostic support when combined with elevation of C-reactive protein, erythrocyte sedimentation rate, and white blood cell count.
3) The clinical evaluation:
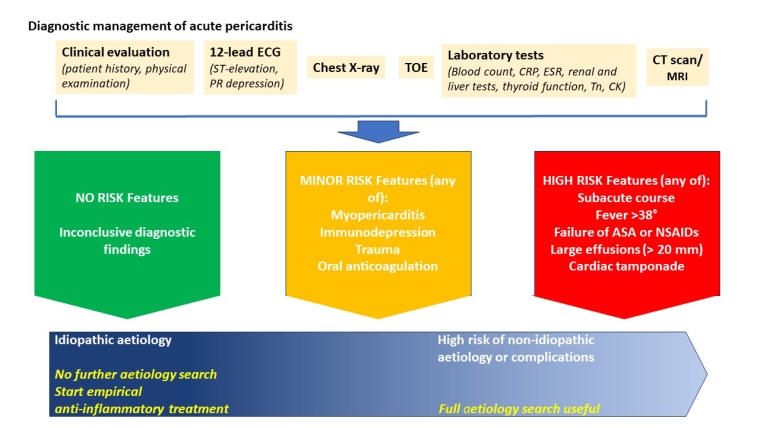
Requires a full diagnostic workup (Central illustration) and diagnosis needs the presence of 2 out of 4 criteria:
• pleuritic chest pain
• ECG changes: widespread ST-elevation, or PR depression, among others
• pericardial friction rubs
• pericardial effusion (newly identified or worsening)
Patients with minor or high-risk features, as described in the Central illustration, require hospital admission and a full aetiology search, while others can follow outpatient check-ups and an empiric trial with NSAIDs without an aetiology search [2].
Central illustration. Diagnostic flow-chart for diagnostic management of acute pericarditis.
ASA: aspirin; CRP: C-reactive protein; CT: computed tomography; ECG: electrocardiogram; ESR: erythrocyte sedimentation rate; MRI: magnetic resonance imaging; NSAID: non-steroid anti-inflammatory drugs; TOE: transoesophageal echocardiogram
4) Patient risk
This diagnostic approach may be followed in an out-patient environment, only requiring hospital admission in cases of Tn elevation or important effusions.
Generally, idiopathic pericarditis is rarely a severe and complex illness and tends to complete remission in a few weeks without complications.
In clinical practice, small pericardial effusions (<5 mm) in totally asymptomatic patients are sometimes found incidentally during imaging tests done for other indications. After a careful exclusion of severe secondary forms, such as an unknown neoplastic condition, these findings may be considered benign and, if the serology is negative, do not require treatment or particular follow-up measures.
Therapeutic ‘tip and tricks’ for idiopathic pericarditis
Therapy mainstay
Acute pericarditis, although generally a benign illness, may cause significant short-term disability due to chest pain and discomfort, may be complicated by large pericardial effusions or tamponade, and may have a significant risk of recurrence.
The mainstay of treatment of pericarditis is represented by anti-inflammatory drugs, which have, however, different profiles in effectiveness and side-effects.
The most common recommended therapies for idiopathic pericarditis are shown in Table 1:
Table 1. Recommended therapy for idiopathic pericarditis.
First-line therapy:
- Aspirin
- Dose: 650 to 1,000 mg, 3 times/day
- Duration: 1 to 2 weeks
- Tapering: Decrease dose by 250 mg per week
- Ibuprofen
- Dose: 600 to 800 mg, 3 times/day
- Duration: 1 to 2 weeks
- Tapering: Decrease dose by 200 mg per week
- Indomethacin
- Dose: 25 to 50 mg, 3 times/day
- Duration: 1 to 2 weeks
- Tapering: Decrease dose by 25 mg per week
- Plus: Colchicine
- Dose: 0.5 to 0.6 mg, 2 times/day
- Duration: 3 months (acute), 6 months or more (recurrent)
- Tapering: Usually not tapered
Second-line therapy (for refractory cases or patients with a contraindication to NSAID therapy):
- Prednisone
- Dose: 0.2 to 0.5 mg/kg per day
- Duration: 2 to 4 weeks (acute or recurrent)
- Tapering: Gradual tapering over 2 to 3 months
- Plus: Colchicine
- Dose: 0.5 to 0.6 mg, 2 times/day
- Duration: 3 months (acute), 6 months (recurrent); generally continued for 4 weeks or more after discontinuation of glucocorticoid
- Tapering: Usually not tapered
Third-line therapy:
- Second-line therapy plus aspirin dosed as for first-line therapy
Fourth-line therapy:
- One of the following agents (or pericardiectomy):
- Rilonacept
- Dose: Loading dose of 320 mg (2 subcutaneous doses of 160 mg on the same day at 2 different sites)
- Maintenance: 160 mg subcutaneously weekly for several months
- Tapering: Slow taper over >3 months
- Anakinra
- Dose: 1 to 2 mg/kg subcutaneously daily (maximum 100 mg daily)
- Duration: Several months
- Tapering: Slow taper over >3 months
- Azathioprine
- Dose: 1 mg/kg orally daily, increasing to 2 to 3 mg/kg daily (maximum 150 mg daily)
- Duration: Several months
- Tapering: Not tapered
- Methotrexate
- Dose: 10–15 mg/week
- Duration: Several months
- Tapering: Not specified
- MMF (Mycophenolate mofetil)
- Dose: 2,000 mg/day
- Duration: Several months
- Tapering: Not specified
- IVIG (Intravenous immunoglobulin)
- Dose: 400 to 500 mg/kg IV per day
- Duration: 5 days (may repeat after 1 month)
- Tapering: Not tapered
CrCl: creatine clearance IVIG: intravenous immunoglobulins; MMR: mycophenolate mofetil
Therapy should be continued according to the timelines shown in the Central illustration.
A serology assessment should be done periodically and may confirm the resolution of the disease.
Therapy should be continued over the suggested timelines if normalisation doesn’t occur.
Colchicine therapy-related problems
Specific instructions about colchicine doses are suggested in these specific conditions:
- Children: ≤5 years 0.5 mg/day, >5 years 1.0–1.5 mg/day in two or three divided dosesl Elderly (>70 years): reduce dose by 50% and consider CrCI
- Renal impairment: CrCI 35–49 mL/min 0.5–0.6 mg once daily, CrCI 10–34 mL/min 0.5-0.6 mg every 2-3 days, CrCI <10 mL/min avoid chronic use of colchicine. Use in serious renal impairment is contraindicated by the manufacturer.
- Hepatic dysfunction: avoid in severe hepatobiliary dysfunction and in patients with hepatic disease.
- Consider dose reduction in case of association with statins (increased myotoxicity), macrolide (decrease colchicine metabolism), ciclosporin (reciprocal enhancement of side effects), verapamil (increases verapamil serum concentration, enhances colchicine nephrotoxicity).
Although colchicine has earned an essential role in idiopathic pericarditis treatment in recent times, it entails important side effects and toxicity.
Colchicine can cause some mild gastrointestinal side effects (in up to 10% of cases) including nausea, vomiting, diarrhoea, abdominal pain, being a common cause of drug withdrawal; these effects usually may resolve with dose reduction.
It’s important to use weight-adjusted doses in order to reduce these side effects. A loading dose was initially used but is now avoided in order to reduce potential gastrointestinal side effects and improve patient compliance. Diarrhoea may be exacerbated by the common concomitant use of antibiotics and proton pump inhibitors.
Other less common side effects include elevation of transaminases and reversible alopecia. In <1 % of cases, other side effects are reported, including bone marrow suppression and myotoxicity.
Recurrent pericarditis therapy
In contrast to a first episode of acute pericarditis, recurrent pericarditis may be problematic condition, difficult to cure.
The recent progress in the study of acute pericarditis allows for a better understanding of the disease and a therapy tailored to the individual patient. However, further research is required to understand questions that remain unsolved.
Recently, in the AIRTRIP study, anakinra, an IL-1 receptor blocker, with targeted therapy against this pivotal cytokine of the innate immunity, showed a high efficacy, alleviation of symptoms, and suggested an essential role for this cytokine in pericardial diseases.
Given the characteristics and the high dosages of the drugs, many patients may experience side effects which may limit tolerance and compliance to the therapy.
When an acute pericarditis is complicated or is not going to remission
When an acute pericarditis shows no kind of remission after 4 to 6 weeks, pericarditis is defined as incessant. It is considered a recurrent pericarditis if there is a new event after a symptom-free interval of 4 to 6 weeks. Chronic pericarditis lasts >3 months. A recurrent form is generally an evolution from acute idiopathic pericarditis. Incessant and chronic forms are more frequently secondary forms. In any case, when pericarditis does not resolve after one month of correct treatment, a careful evaluation is required to exclude a secondary form.
Tamponade
As alluded to in the article, (on "Secondary pericarditis" by Iris Parrini and Elena Coletti Moia) any kind of evolution is generally related to the aetiology of the pericarditis.
The probability of tamponade is strictly related to the impairment between fluid production and drainage velocity. The former depends on the seriousness of inflammation which in turn leads to a severe degree of vessel permeability and rapid transition of liquid into the pericardial sac, and/or eventually bleeding i.e., of a pericardial metastasis; the latter is conditioned by the function of the lymphatic drainage system.
It has been evaluated that about 30% of acute tamponade requiring drainage are due to a neoplastic form.
Chronic forms and constrictive forms
Any aetiology related to an infectious or inflammatory disease may, through a chronic inflammatory persistent condition, lead to a fibrous reaction and to the thickening of the pericardial leaflets. The kind of pericardial fluid (transudate vs. exudate) heavily influences the possible chronic evolution.
How to distinguish incessant, recurrent and chronic pericarditis from the secondary forms and the most probable secondary forms
The epidemiological, clinical, serologic characteristics are generally good indicators compared to the correct aetiology (See the article, [on "Secondary pericarditis" by Iris Parrini and Elena Coletti Moia] and the Central illustration).
Generally, the diagnostic process is easy and linear, but some cases have a complicated and difficult diagnostic path, which requires, among other issues, a strong collaboration with the imaging expert who may suggest the help of magnetic resonance imaging (MRI) or a CT scan over a ‘common’ echocardiography.
Every effort must be made by the cardiologist who has a patient with suspected secondary pericarditis, given that many forms of these illnesses have potentially poor prognostic implications.
Conclusions
While acute idiopathic pericarditis is the most common presentation of pericardial diseases and generally has a benign course, secondary pericarditis can have lots of complications and recurrences and, moreover, may be associated with extremely serious infectious and non-infectious illnesses.
Secondary pericarditis requires, as a consequence, an in-depth clinical process to identify them, and to reach the correct aetiologic identification which in turn allows for the best possible treatment.
Currently, the patient’s history, through the analysis of conditions that favour the development of pericarditis, the exclusion or confirmation of internal medicine pathologies (cancer!), geographical exposures (TB!), are the mainstays of the diagnostic process.
The second essential great help in the diagnosis and guidance for tailored treatment are the new imaging studies. When echocardiography is not the solution, a CT scan or MRI may lead to a clearer definition of the situation.
Awareness of the diagnostic and aetiologic features of pericarditis is key to proper treatment and the prevention of complications.
In patients with recurrent or constrictive pericarditis or in those dependent on corticosteroids, targeted therapies with IL-1 blockers or other immunomodulators represent promising therapies.
Note to editors
Authors:
Antonella Fava1, MD; Davide Forno2, MD
- Division of Cardiology, Cardiovascular and Thoracic Department, "Citta della Salute e della Scienza" Hospital, Turin, Italy;
- Cardiology Department, Maria Vittoria Hospital, ASL Città di Torino, Turin, Italy
Address for correspondence:
Dr. Antonella Fava, corso Marconi 2, 10125 Torino, Italy
Author disclosures:
The authors have no conflicts of interest to disclose.
References
- Brucato A, Imazio M, Cremer PC, Adler Y, Maisch B, Lazaros G, Gattorno M, Caforio ALP, Marcolongo R, Emmi G, Martini A, Klein AL. Recurrent pericarditis: still idiopathic? The pros and cons of a well-honoured term.Intern Emerg Med. 2018;13:839-844.
- Adler Y, Charron P, Imazio M, Badano L, Barón-Esquivias G, Bogaert J, Brucato A, Gueret P, Klingel K, Lionis C, Maisch B, Mayosi B, Pavie A, Ristic AD, Sabaté Tenas M, Seferovic P, Swedberg K, Tomkowski W; ESC Scientific Document Group. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS).Eur Heart J. 2015;36:2921-64.