Definition of aortic dilatation
In the context of genetic diseases of the aorta, a correct definition of aortic pathology is needed both in terms of diagnosis and treatment. When considering further work-up for genetic causes, it is important to define aortic dilatation and -aneurysm. Aortic dilatation in most genetic aortic disease entities is typically located at the root, at the level of the sinuses of Valsalva and is defined as a measured aortic diameter above the 95% confidence interval of the normal distribution in a large reference population. (1) (2).
To correlate measured aortic diameters with normal values, age- and body surface area (BSA)-related nomograms for upper limit of normal (ULN) or equations for z-score calculation should be used. The z-score is a standard numerical representation on how much a specific value defers from the average in a normalized distribution. A z-score of 0 means that the studied value coincides with the mean. Normal z-scores range from -2 to +2 standard deviations. Positive z-scores indicate that the value is above average while negative z-scores indicate that the value is below average. The z-score can be calculated using the formula z=(x- µ)/ σ were x is the studied value, µ is the mean and σ the standard deviation. A z-score ≥2 indicates a value exceeding two standard deviations (the 95% confidence interval).
Z-scores correlate with percentiles. Percentiles show the ranking of a value in a set of 100 equal parts. A z-score of 0 corresponds to the 50th percentile while z-scores of 2 and 3 correspond to the 97,7th and 99,9th percentile respectively. The upper limit of normal (ULN) is usually set at the 95th percentile.
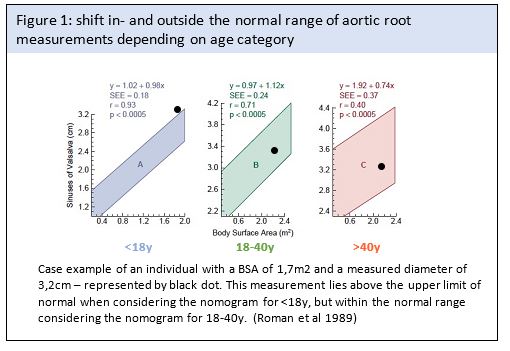
The first nomograms for normalizing aortic root diameters (at the level of the sinuses of Valsalva and the supra-aortic ridge) with 2D echocardiography were established by Roman and colleagues in 1989 (3) . In this study 135 adults and 52 children were included and the ULN was defined based on BSA. These nomograms, which are widely used in clinical practice and adopted in guidelines, made a subdivision in three different age categories, leading to jumps in diameter prediction when transitioning from one age category to the next one, as illustrated in figure 1.
This problem was resolved in the updated nomograms by the same group for aortic root ULN
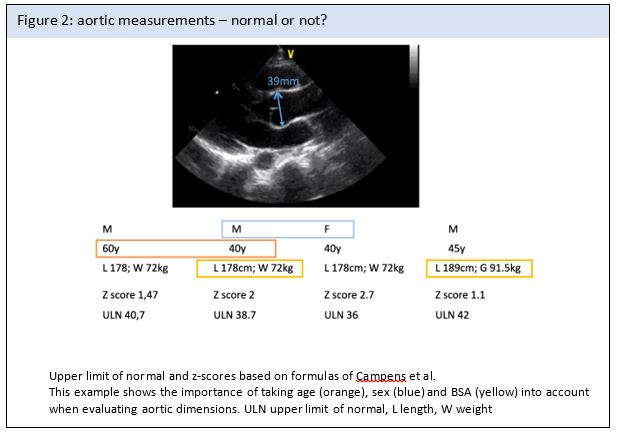
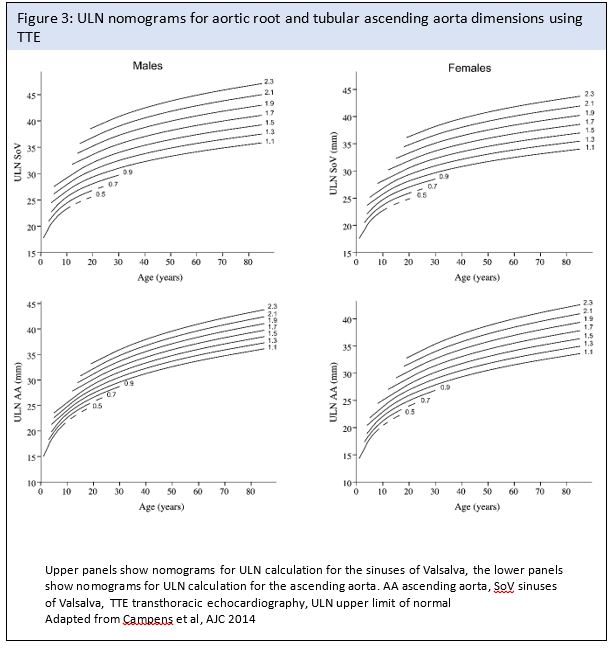
prediction, considering age as a continuous variable(4). Meanwhile, several other aortic nomograms have been developed. Nomograms are derived from regression equations including age, sex and bsa as the most common variables. Figure 2 illustrates the importance of taking these factors into account and an illustration of nomograms in which obtained values can be correlated with expected values is provided in Figure 3 (Figure 2&3).