Take-home messages
- TR is a common valvular disease and has an important impact on functional capacity and clinical outcomes.
- Early referral for the evaluation of a TR intervention (transcatheter or surgery) is essential to improve symptoms and quality of life.
- Detailed anatomical assessment by multimodality imaging of the tricuspid valve is essential.
- A comprehensive approach to evaluate patients with TR regarding clinical assessment and imaging is needed.
Introduction
Tricuspid regurgitation (TR) is a common finding during routine echocardiography [1]. Mild TR is detected in 75% of adults, while relevant (≥moderate) TR is estimated to affect 4% of the population over 75 years of age, which is comparable to the prevalence of aortic stenosis and mitral regurgitation [1-3]. For yet unknown reasons and in contrast to other valvular diseases, women are up to four times more frequently affected than men and the female sex is an independent predictor of the severity and progression of the disease [4-6]. This may be due to a higher prevalence of atrial fibrillation and heart failure with preserved ejection fraction (HFpEF) [7]. Besides age, sex and atrial fibrillation, pre- and postcapillary pulmonary hypertension are predictors of disease severity and progress [8].
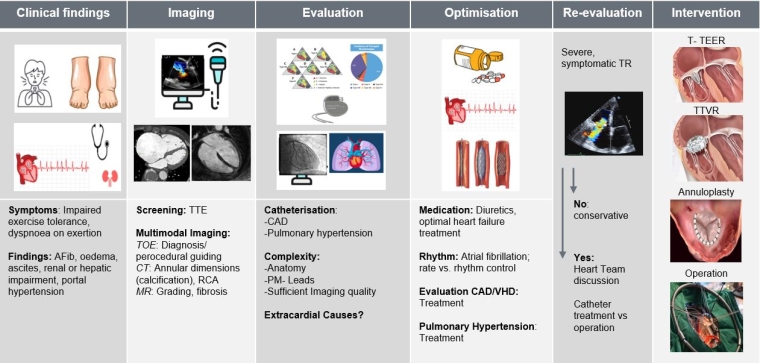
TR manifests with impaired functional capacity and dyspnoea on exertion, as well as peripheral oedema, ascites, gastrointestinal symptoms and right heart failure, and in the advanced stages, consecutive renal and liver dysfunction [9]. The first therapeutic measure consists of the initiation of diuretic treatment.
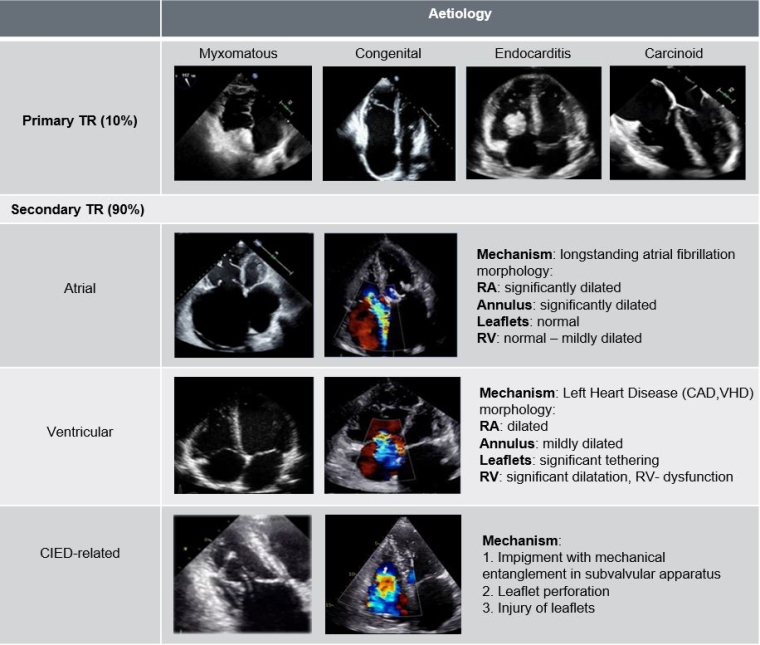
Because of the longstanding and misleading belief that the treatment of left-sided heart disease improves TR in the majority of patients and that TR does not contribute to clinical symptoms and long-term outcomes, research on this topic has been scarce in the past [9,10]. In recent years, evidence has accumulated that significant TR is associated with an increased mortality of 40-70% after 1-4 years, even when adjusted for comorbidities [11-14]. These mortality rates are comparable to aortic stenosis [15] and results have been replicated in different study cohorts, applying not only to patients with isolated TR but also to patients with heart failure with reduced ejection fraction (HFrEF) [16].
Despite increasing evidence, TR remains a rarely assessed and treated valve disease and patients are often referred too late, when irreversible right heart failure is present and subsequent treatment is associated with increased operative risk.