















Abbreviation list
CV: cardiovascular
CVD: cardiovascular disease
IBD: inflammatory bowel disease
Take-home messages
- Cardiovascular disease is the leading cause of death in women all over the world.
- Multidisciplinary, integrated, and dedicated paths for females are currently lacking.
- Cardiovascular risk is usually underestimated in women. Risk assessment in women should incorporate reproductive and pregnancy history, comorbidities, and psychosocial conditions
Patient-oriented messages
- Prevention of cardiovascular disease in women should start at childbearing age and continue through all the phases of life.
- Awareness of an individual’s cardiovascular risk and of the clinical presentation of cardiovascular disease is a mainstay of primary prevention.
- Traditional risk factors have a stronger impact on women’s cardiovascular health, and sex-specific conditions are major risk enhancers.
Impact on practice statement
Cardiovascular disease is the number one killer of women worldwide. Yet women, with their ability to give life and their traditional and implicit caregiver role, deserve greater recognition of their value from a psychosocial point of view. Prevention is of paramount importance.
Key messages include:
- Consider how a woman’s age relates to her cardiovascular risk and act accordingly.
- Educating women regarding their risk, atypical symptoms, and correct reporting of symptoms may help reduce the gender gap.
Introduction
Cardiovascular (CV) disease is and remains the number one killer of women worldwide, accounting for approximately one in three female deaths. Sadly, although age-standardised cardiovascular mortality has reduced over the years, it has declined less in females than in males [1]. This may be related to the persistent pharmacological and invasive undertreatment of women. However, women who require medical attention are older, with more comorbidities than men, so each woman’s cardiovascular story starts well before she seeks treatment. Indeed, the traditional misconception of cardiovascular disease being a predominantly male disease has delayed advances in prevention and care for women, which is far from ideal. The sex-based biological differences and gender-related social factors point to a need for tailored prevention strategies that target the female-specific risk factors and that prevent the delayed identification and/or the misinterpretation of symptoms. It is important to note that true prevention starts during the childbearing years, or even before. This article was written by a female interventional and clinical cardiologist passionately dedicated to the effective and holistic care of her female patients.
Gender cardiology and cardiovascular risk
Cardiology is one of the best examples of gender medicine. Indeed, gender-based cardiology includes all branches of internal medicine (Figure 1). To ensure true primary prevention, the network of these specialists should be in constant communication, just as the petals of a flower surround its centre (it is not by chance that the centre of a flower is called the gynoecium).
Figure 1. The flower of gender cardiology. Most of the depicted diseases are more frequent or require special attention in women, including cardiological evaluation.
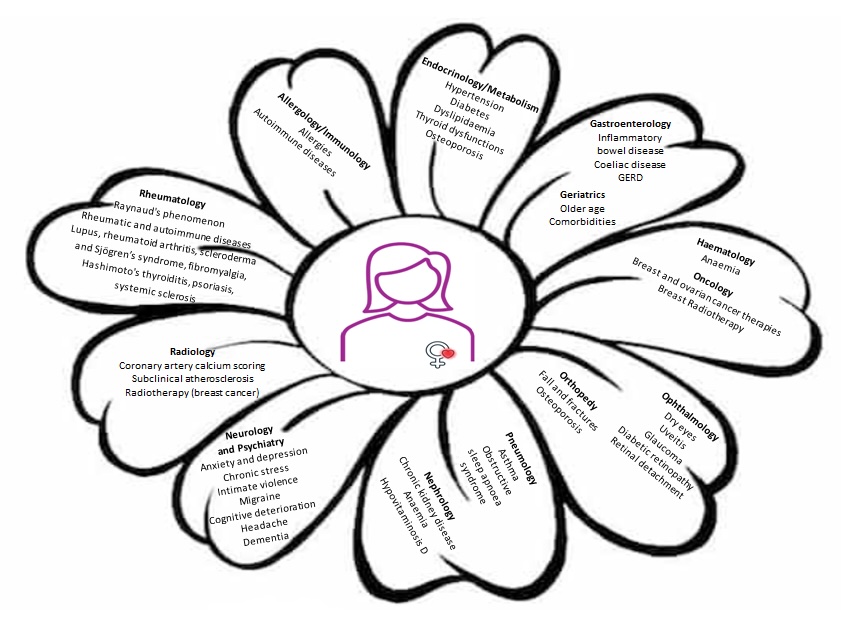
GERD: gastroesophageal reflux disease
The male sex represents a well-recognised cardiovascular risk factor per se, and men are managed accordingly. For women, the situation is different. Medical attention is sought less frequently and more often later in life in women than in men. Moreover, the primary physician or the emergency care room usually remains the only ones who takes charge of a woman’s health. However, only relying on the primary physician or emergency access might result in a lack of recognition or exploration of various important aspects connected to higher cardiovascular risk, if this medical attention is not extended beyond the occasional request. This common behaviour of women worsens the already existing systematic delays in diagnosis and treatment of women with cardiovascular disease.
Traditional cardiovascular risk factors
Traditional CV risk factors are often overlooked and undertreated in women, despite their stronger impact on women’s overall cardiovascular risk as compared with men. Hypertension is more frequent in women and is a strong predictor of stroke and heart failure. Diabetes confers a higher cardiovascular risk in women as compared to men (4-fold vs 2.5-fold) [2]. As a rule, any diabetic woman should undergo an early cardiology evaluation. Of note, microvascular complications of diabetes, such as retinopathy, neuropathy, and nephropathy, should be detected in advance since they are indices of a worse prognosis. A fundus oculi examination should be routinely performed in every diabetic woman, and it should be performed early in patients with a history of gestational diabetes.
Although smoking remains less common in women, it has a stronger impact on women’s risk of cardiovascular events (3.3- vs 1.9-fold). Indeed, when comparing the same number of cigarettes smoked by women and men, the CV risk factor is 5 times greater for women. In short, women experience the same level of harm after smoking one-third the number of cigarettes smoked by men [3].
When defining low-density lipoprotein targets, it is important to take into account adjunctive factors, called “risk modifiers” (premature menopause, pre-eclampsia or hypertension during pregnancy, chronic autoimmune and inflammatory disorders, social deprivation, stress, major psychiatric disorders, obesity and physical inactivity, etc.), to correctly identify the female CV risk class and proceed with early preventive therapies [4].
Female-specific and predominant risk factors
Several risk factors are unique to, or more common in, women. Besides factors directly connected with hormonal profiles and pregnancy, other morbid conditions independently contribute to cardiovascular risk.
Endocrinologic and metabolic diseases
Thyroid dysfunctions (and cancer) are significantly more frequent in women. Both hyper- and hypothyroidism have a direct impact on cardiac health. Osteoporosis is also more frequent in women, and it is mostly due to the oestrogen decline during menopause. It should be recognised and treated not only by administering vitamin D, but also by considering hormone replacement therapy. Pathological fractures may lead to a need for prolonged bed rest with an increased risk of pulmonary embolism. Hypovitaminosis D is, per se, a cardiovascular risk factor [5], besides its detrimental effect on the mood, which may worsen depressive tendencies. Nearly a third of women worldwide are obese [1], and obesity, especially central obesity, is a well-known CV risk factor.
Strict or uncontrolled dietary regimens, with a possible use of diuretics to lower bodyweight and “fit the dress,” may represent an additional CV risk in women. Some dietary supplements or algae may contain thyroid hormones to promote weight loss, and these may have a detrimental impact on the heart. Additionally, eating disorders such as anorexia, bulimia, and binge eating, which are more frequent in women, increase CV risk.
Autoimmune diseases
Autoimmune and inflammatory diseases are far more frequent in women than in men. Lupus and rheumatoid arthritis double the cardiovascular risk [6], both because of the condition itself and its treatment. For example, prolonged and chronic corticosteroid treatment increases the risk of hypertension and diabetes, thus worsening the CV profile. Moreover, scleroderma and Sjögren’s syndrome are often associated with precapillary pulmonary hypertension, which requires prompt identification and treatment.
Kidney and gastrointestinal diseases
Chronic kidney disease is more frequent in females than in males and is a well-known independent risk factor for CV diseases.
Similarly, inflammatory bowel disease (IBD) and coeliac disease are more frequent in women and increase cardiovascular risk per se due to both the chronic inflammatory state they cause and their treatment. IBD can also cause anaemia, hypovitaminosis D, infertility, and, of course, depression. A gluten-free diet may be rich in processed foods with sweeteners and saturated fats, which are potentially harmful and lead to a higher risk of developing dyslipidaemia and diabetes in coeliac patients [7].
Cholelithiasis is more frequent in women, and together with dyspepsia may mimic cardiac symptoms.
Pulmonary diseases
Asthma is more frequent in women, but any dyspnoea in a woman should not be overlooked. It might be an angina equivalent or be caused by valvular heart disease or previous/current pulmonary embolism. Cardiology evaluation and echocardiography may be helpful for a differential diagnosis. Also, prolonged treatment of asthma with ß-agonists may enhance cardiovascular risk. Nasal spray with α-stimulators may increase CV risk as well. Obstructive sleep apnoea syndrome in postmenopausal women is as frequent as in men but is often overlooked.
Neurological and psychiatric diseases
Anxiety and depression are twice as common in women than in men, and the correlation with increased CV risk is well known [8]. Similarly, chronic stress, caregiving burdens, and exposure to intimate partner violence are more prevalent in women. These conditions may also interfere with the possibility of seeking medical attention and compliance with therapy, further worsening the clinical scenario. Too often, these scenarios are underestimated and under-recognised.
I have a personal method that can be helpful to rule out depression when a patient, especially a woman, comes to the cath lab. I ask her to tell me about the best moment in her life. If only anxiety is present, it is quickly overcome when answering this question. Conversely, in depressed patients, it takes longer for the patient to answer.
Antidepressant and antipsychotic drugs should be taken under medical control and not abused. The QTc interval should be monitored during treatment using the sex-specific cut-off (pathological QTc >460-470 ms in women). Notably, electrolyte imbalances (hypokalaemia, hypocalcaemia) caused by diuretics or disorders such as anorexia/bulimia contribute to QTc prolongation.
Migraines are more frequent in women. Very often, these patients are not even sent to a neurologist, let alone to a cardiologist, and yet, these same migraines and headaches can be associated with hypertension, cerebrovascular disease, and a patent foramen ovale. Similarly, what is often diagnosed as dementia or Alzheimer’s disease (which is also more frequent in women) may have a cerebrovascular origin, and untreated atrial fibrillation may coexist with these conditions. Referral to a cardiologist is critical in these cases. Dementia itself increases CV risk, and cognitive deterioration seems to increase in postmenopausal women.
Orthopaedic problems
Women are more prone to a sedentary lifestyle and osteoarticular problems at all ages. Bone fractures are more frequent in ageing women, especially post-menopause, due to osteoporosis. The abuse of non-steroidal anti-inflammatory drugs (NSAIDs) for these reasons may increase CV risk.
Ophthalmological problems
The presence of retinal holes and detachment may be connected to diabetes and hypertension. Dry eyes and uveitis are more frequent in women, and patients presenting with these conditions should be screened for pulmonary hypertension. Closed-angle glaucoma, which also increases CV risk, is more frequent in women and requires modulating beta-blocker therapy [9].
Ageing and comorbidities
In general, women live longer than men and frequently have more comorbidities later in life. Health does not improve with age, and women are also increasingly less inclined to seek medical attention than men. A geriatrician who coordinates treatment paths for older women would be useful. Indeed, in the absence of caregivers and familial support, “silent” and untreated heart disease becomes even more frequent. Despite a strong desire for independence, older women should never be “left alone” without medical and social attention, especially after family care has ended.
This overview of comorbidities specifically increasing women’s CV risk is not exhaustive, but gives an idea of how many conditions are interconnected and may carry a hidden high or very high CV risk. Therefore, a comprehensive approach should be used when considering CVD prevention in females.
“Part 2. Gender specific issues” and conclusion: to be published next month.
