Keywords
chronic coronary syndrome, diagnostic pathways, non-invasive imaging, pre-test probability, risk stratification
Abbreviation list:
AHA/ACC: American Heart Association/American College of Cardiology
CAD: coronary artery disease
CCTA: coronary computed tomography angiography
CMR: cardiac magnetic resonance
CCS: chronic coronary syndrome
ECG: electrocardiogram
ESC: European Society of Cardiology
MPI: myocardial perfusion imaging
PTP: pre-test probability
Take-home messages
- Pre-test probability (PTP) assessment is essential in guiding diagnostic decisions for suspected CCS, reducing unnecessary testing.
- A patient-centred approach integrating symptoms, risk factors, and imaging results enhances clinical decision-making.
- Non-invasive imaging modalities, such as CCTA, MPI, and CMR, are pivotal in diagnosing and risk stratifying patients.
- Future advancements, including artificial intelligence and novel biomarkers, may refine diagnostic accuracy and personalised CCS management.
Impact on practice
Accurate risk stratification and pre-test probability assessment are fundamental in the initial evaluation of suspected chronic coronary syndrome. Incorporating a multimodality imaging approach helps tailor diagnostic strategies, reducing unnecessary invasive procedures while ensuring timely intervention in high-risk patients. Clinicians must balance guideline recommendations with individual patient profiles to optimise care. Understanding the strengths and limitations of different diagnostic tools can enhance early disease detection, improve clinical outcomes, and refine healthcare resource allocation.
Patient-oriented message
Patients experiencing symptoms like chest discomfort, shortness of breath, or fatigue may require an evaluation for CCS—a condition related to reduced blood flow to the heart. To begin, you and your physician may have a detailed discussion about symptoms, medical history, and risk factors like high blood pressure, diabetes, or smoking. Based on this, your physician will estimate the likelihood of significant heart artery disease using a pre-test probability (PTP) assessment, which helps guide the next steps. Lifestyle changes and regular monitoring may be recommended if your risk is low. If your risk level is higher, further tests—such as heart scans or stress tests—may be needed to assess blood flow to the heart. The goal is to ensure that patients receive the proper care while avoiding unnecessary tests and procedures.
Introduction
Chronic coronary syndrome (CCS) poses a significant public health challenge, encompassing a range of clinical manifestations associated with coronary artery disease (CAD). The latest guidelines from the European Society of Cardiology (ESC) have reshaped the diagnostic and management strategies for CCS, highlighting the necessity of precise risk stratification and individualised treatment approaches [1]. This article seeks to consolidate current insights on the initial clinical evaluation and diagnostic probability assessment of suspected CCS cases, focusing on the most recent evidence-based guidelines and diagnostic techniques.
Understanding chronic coronary syndrome
CCS includes a range of clinical presentations of CAD, such as stable angina and silent ischemia, which, if not properly managed, can result in substantial morbidity and mortality [2]. The ESC guidelines have transitioned from using the term "stable CAD" to "chronic coronary syndrome" to highlight the continuous risk of adverse cardiovascular events in these patients [3]. This revision reinforces the need for thorough assessment and personalised management strategies tailored to each patient's profile.
Initial clinical assessment
The initial evaluation of patients with suspected CCS starts with a detailed discussion with the patient about the symptoms, medical history, risk factors, the identification of potential comorbidities and physical examination [4]. CCS symptoms can vary widely, contributing to underdiagnosis or misdiagnosis if not thoroughly assessed [2]. A comprehensive understanding of the patient's clinical presentation, including atypical manifestations, is essential for accurate diagnosis and effective management. Based on this, the doctor will estimate the likelihood of significant heart artery disease using a pre-test probability (PTP) assessment, which guides the next steps [4].
Risk stratification and diagnostic probability assessment
The ESC guidelines advocate using a PTP assessment to classify patients based on their likelihood of having obstructive CAD [3]. This approach considers clinical factors such as age, sex, and symptom characteristics to inform subsequent diagnostic decisions. For example, patients with a high PTP may require invasive testing, whereas those with a low PTP may be managed conservatively [5].
Recent studies have validated the updated PTP models, confirming their effectiveness in clinical practice [3]. Additionally, coronary artery calcium scoring (CACS) has been proposed as a valuable tool for risk stratification, especially in asymptomatic individuals with CAD risk factors [6]. However, current guidelines do not universally endorse CACS for all patients, emphasising the importance of individualised assessment based on clinical context [6].
Pre-test probability
Understanding PTP
In the context of CCS, PTP plays a vital role in guiding the appropriate diagnostic approach [7]. Based on clinical factors such as age, sex, symptom presentation, and risk factors, the ESC guidelines classify PTP into three categories: low (<5%), intermediate (5–15%), and high (>15%) [7]. Note that the 2019 ESC guidelines revised the PTP thresholds, with low risk from 15% to 5% [7]. Additionally, the updated guidelines highlight the importance of combining clinical judgment with validated scoring models, such as the Diamond-Forrester model, to improve the accuracy of PTP assessment [8].
Clinical factors influencing PTP assessment
Age and sex are among the strongest predictors of CCS, as CAD prevalence rises with age and differs between sexes [8]. For example, younger women often present with atypical symptoms, which can contribute to underdiagnosis, whereas older men are more likely to experience classic angina symptoms [2].
Symptom presentation is another key determinant, with patients exhibiting typical angina having a higher PTP compared to those with atypical symptoms [9]. Additionally, traditional risk factors such as hypertension, diabetes, hyperlipidaemia, and smoking further increase the probability of CAD [2]. Incorporating these factors into PTP assessment enables a more individualised approach to diagnosis and management.
Diagnostic testing based on PTP assessment
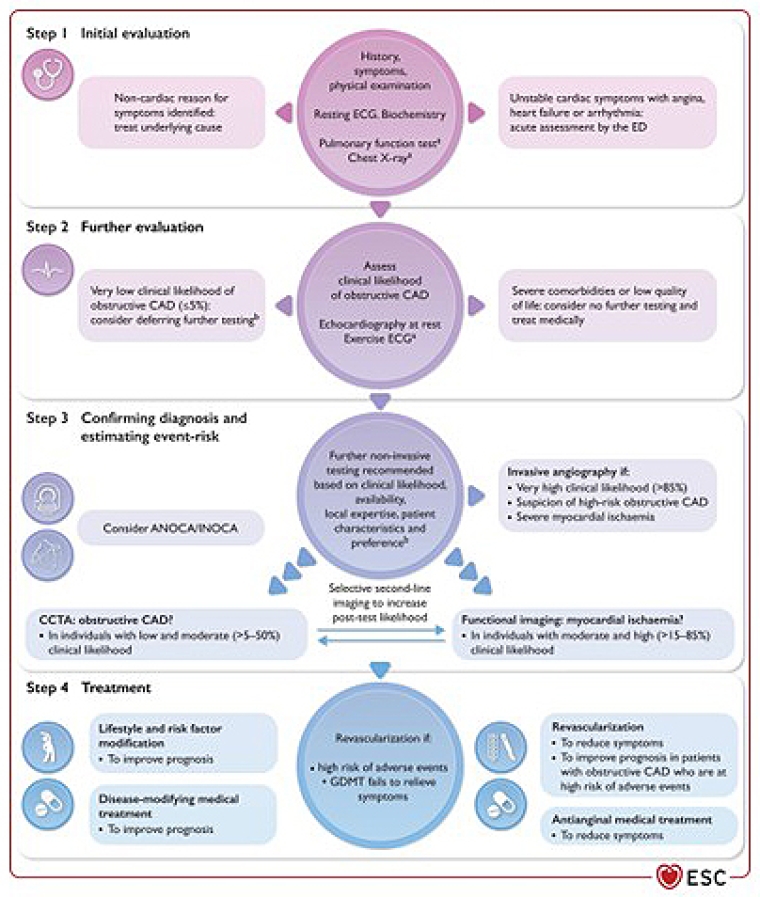
The ESC guidelines recommend a stepwise approach to diagnostic testing based on the PTP assessment. For patients with low PTP, non-invasive testing may not be necessary, and clinicians can consider a conservative management approach [9]. In contrast, an intermediate or high PTP, should lead to further diagnostic evaluation to confirm or exclude the presence of obstructive CAD.
Non-invasive imaging modalities, such as coronary computed tomography angiography (CCTA) and functional imaging tests (e.g., stress echocardiography and myocardial perfusion imaging), are recommended for patients with intermediate to high PTP [10]. These tests provide valuable information regarding the presence and extent of coronary artery disease, guiding subsequent management decisions.
Role of non-invasive imaging in PTP assessment
Non-invasive imaging is crucial in evaluating patients with suspected CCS, especially those with intermediate PTP. CCTA has become a first-line diagnostic tool due to its high sensitivity and specificity in detecting obstructive CAD, allowing for effective risk stratification [10].
Functional imaging tests, such as stress echocardiography and myocardial perfusion imaging, are valuable for assessing myocardial ischaemia [10]. These modalities help evaluate the functional significance of coronary lesions, which is essential for guiding treatment strategies.
Impact of comorbidities on PTP assessment
Conditions such as diabetes, chronic kidney disease, and peripheral artery disease are linked to a higher risk of adverse cardiovascular events [2]. These comorbidities require a more thorough evaluation of the patient's overall cardiovascular risk profile, which can influence the interpretation of PTP and the choice of subsequent diagnostic tests.
For example, patients with chronic kidney disease often have elevated troponin levels, which can complicate the assessment of myocardial injury and require careful interpretation of diagnostic findings [9]. Likewise, diabetes can modify the typical presentation of angina, increasing the risk of underdiagnosing CAD in this population [2].
Challenges in PTP assessment
Despite advancements in PTP assessment, several challenges persist. Variability in clinical practice, differences in patient populations, and the subjective nature of clinical judgment can contribute to inconsistencies in PTP evaluations [9]. Additionally, relying solely on traditional risk factors may not fully account for the complexity of CAD, particularly in women and younger patients [8].
Incorporating novel biomarkers and advanced imaging techniques can improve the accuracy of PTP assessments and enhance risk stratification in these challenging cases [9]. Further research is necessary to validate these approaches and develop standardised protocols for PTP assessment across diverse patient populations.
Future directions in PTP assessment
Future research should aim to refine PTP assessment methods and investigate the potential of emerging diagnostic technologies. Integrating artificial intelligence and machine learning algorithms into risk stratification models may enhance the precision of PTP assessments and support personalised treatment approaches [7].
Developing comprehensive risk assessment tools that combine clinical, imaging, and biomarker data could offer a more holistic evaluation of a patient’s cardiovascular risk profile [9]. and empower clinicians to make well-informed decisions regarding diagnostic testing.
Finally, the pre-test probability assessment plays a key role in guiding clinical decisions and management strategies. The ESC guidelines offer a comprehensive framework for PTP assessment, highlighting the need to incorporate clinical factors, validated scoring models, and non-invasive imaging techniques.