















Keywords
ancient medicine, cardiac physiology, clinical reasoning, heart function, historical cardiology, physiological integration
Take-home messages
- A common cardiocentric theory of human physiology united Hippocratic and Aristotelian medicine.
- Hippocratic cardiocentrism arose from clinical observation, prognosis, and holistic patient assessment.
- The foundations of Aristotelian cardiocentrism were its biological aims and causal explanations.
- Cardiocentrism functioned as a productive organising principle rather than a simple physical mistake.
- This dual legacy of observation and causality is still reflected in contemporary clinical reasoning.
Impact on practice
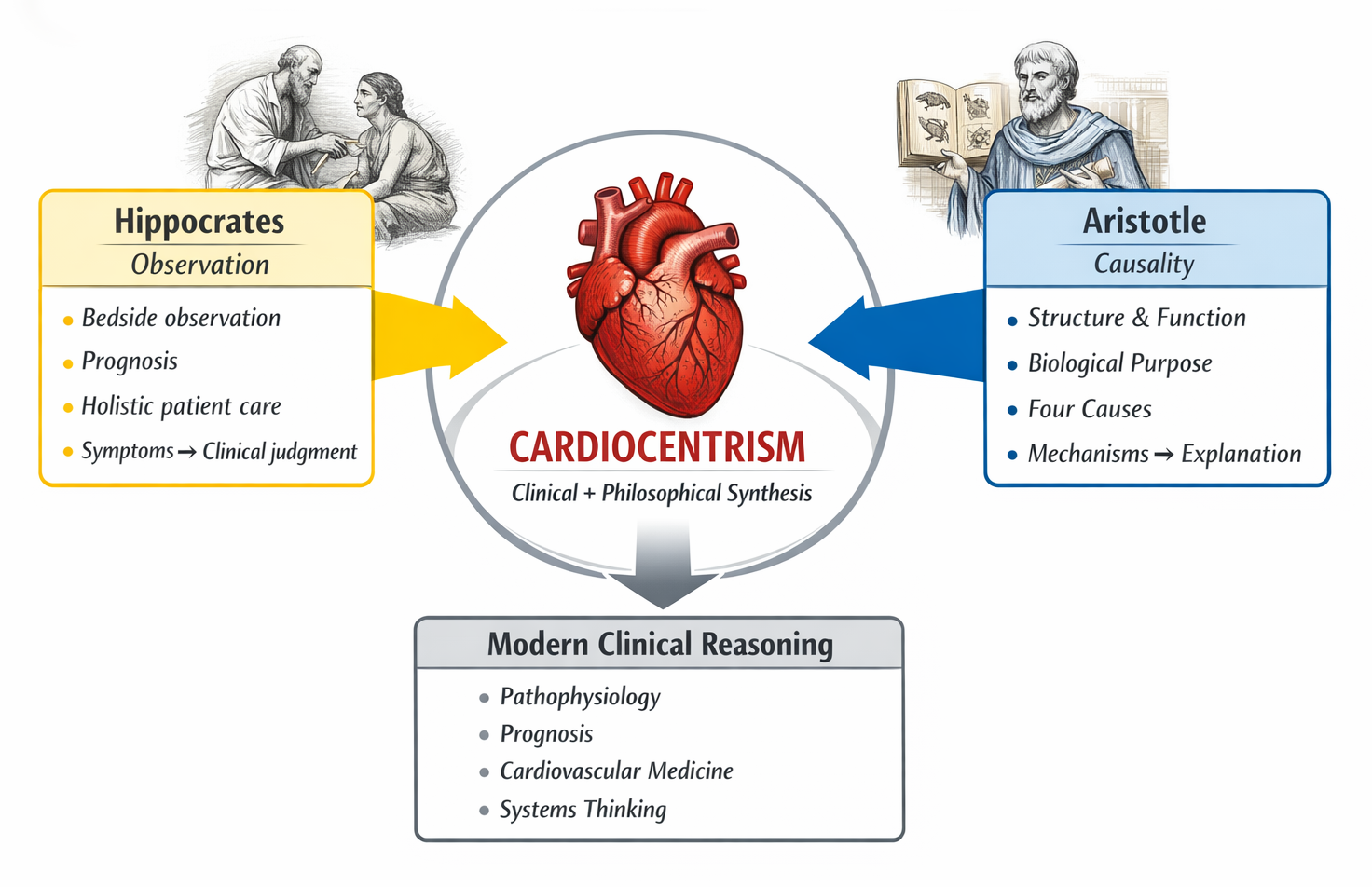
It's probably more fruitful to think of modern medicine as the product of synthesis rather than enmity. The framework for understanding life and causality that comes out of Aristotelian philosophy has been long-lived, as has that of Hippocratic medicine, which began with observation, prognosis, and holistic treatment. One of the central concepts that continues to guide contemporary therapeutic thinking is cardiocentrism. While we have advanced in our understanding of anatomy, the heart remains fundamental to prognosis, systemic integration, and experience. Recognising the cardiocentric roots of medicine reinforces the enduring value of integrating causal reasoning, observational evidence, and engaged patients.
Figure 1. Cardiocentrism as a conceptual bridge between ancient medicine and modern clinical reasoning.
Introduction: medicine between observation and philosophy
Western medicine, like all indigenous systems of healing, grew out of interactive social experiences and the development of rational argumentation, rather than a single process of “intellectual discovery” [1]. Hippocrates and Aristotle are the central figures in this creative process. On the one hand, Hippocrates has often been portrayed as the empiricist absorbed in bedside data; while Aristotle, by contrast, represents a philosopher looking for causal accounts of nature [2,3]. This apparent difference in their approach to knowledge (clinical or otherwise) can obscure a more complex and effective partnership.
Hippocrates was born on the island of Kos between 460 and 370 BCE and is considered the father of western medicine (Figure 2). Members of the Hippocratic Corpus endorsed prognosis, bedside observation, and ethical obligation. Hippocrates was inclined to natural and not supernatural aetiologies of illness, i.e., environmental and physical causes [4,5]. His method transformed medicine from an art to a technē (Greek: τέχvη), which is a hands-on, hard skill based on experience and patient care.
Figure 2. Hippocrates, engraving by Peter Paul Rubens, 1638.
Aristotle (384-322), the philosopher whose ideas helped shape the course of ancient science and medicine, was born in Stagira, Macedonia. Although he was not a doctor, his works on biology provide an all-encompassing system for the comprehension of the structure, function, and causality of lifeforms [2,3] (Figure 3).
Figure 3. Aristotle. Roman copy in marble after a Greek bronze original from 330 BCE.
Despite differing philosophical and methodological approaches, both systems shared a cardiocentric model of human life, in which the heart was believed to be essential for vitality, movement, and the manifestation of illness [6]. Cardiocentrism was not simply an anatomical assertion, however; it offered a philosophical basis that related clinical observation to a more complete interpretation of biological processes. The evolutionary roots and continued allure of such a popular view are important to appreciate in terms of the theoretical underpinnings of contemporary clinical reasoning, especially within cardiovascular medicine [6,7].
Hippocratic medicine: observation, prognosis, and the cardiocentric patient
The medicine of Hippocrates was a decisive, enduring divorce from the religious and mythological interpretation of pathology. Diseases had natural explanations in the humours, exterior conditions, and ways of life [4,8]. This changed climate led to the evolution in concepts of clinical responsibility and rational therapeutics.
The medicine of the late prehistoric and early historic periods is known as Hippocratic medicine, as it was practiced by the enigmatic “father of Western medicine”, Hippocrates. His approach to teaching physicians addressed symptoms, physical findings, timelines, and patient narratives. Prognosis, the prediction about how a disease will develop and end, became an obligation and can be seen as an essential building block in the creation of the modern medical profession – adopting an approach that contributed to strengthening the confidence in both the patients and the doctors themselves [4]. The heart held a special place in this observational framework. Hippocratic texts provide remarkably clear clinical descriptions of circulatory collapse, palpitations, chest discomfort, dyspnoea, and unexpected death [4,8]. These descriptions reveal an intuitive understanding that heart problems frequently signify serious systemic decline. Crucially, Hippocratic cardiology understood heart symptoms as signs of an imbalance affecting the entire body as a single system [8].
Hippocrates acknowledged the brain as the organ in charge of consciousness, thinking, and sensation all at the same time. The brain is referred to as the seat of perception and mental activity in works like On the Sacred Disease [5,8]. However, the clinical primacy of the heart remained crucial for comprehending vitality, systemic collapse, and prognosis, despite this neurocentric component.
The heart in Hippocratic clinical descriptions
Some of the first organised clinical descriptions of cardiovascular pathology can be found in Hippocratic texts. Exertional and resting dyspnoea, oedema, palpitations, abrupt collapse, and radial-induced chest discomfort are all often reported and contextualised within the course of the disease [4,8].
The Hippocratic Corpus contains references to the heart, but the only treatise that focuses exclusively on the structure and motion of the heart is “On the Heart”. The heart's relationship to the vessels, its rhythmic motion, and its connection to breathing and vitality are all discussed in this text. Additional clinical descriptions of cardiac symptoms, such as dyspnoea, collapse, and sudden death, may be found in treatises like “On Diseases” and “Aphorisms”, where heart problems serve as important markers of prognosis and systemic deterioration [4,5,8].
Hippocratic cardiocentrism is distinguished by three characteristics: because acute cardiac symptoms often precede death, the heart was first acknowledged as being vital for maintaining life [4,8]. Second, cardiac symptoms were considered dynamic and impacted by activity, rest, and environmental circumstances [4,8]. Third, the heart's key physiological role was reinforced by its strong relationship to breathing, circulation, and vitality [6,8].
Despite their lack of in-depth anatomical understanding, Hippocratic physicians’ clinical reasoning foresaw eventual ideas on heart disease. More significantly, they developed a diagnostic and prognostic pattern that continues to be essential to modern cardiology, wherein medical judgment was based on heart-related symptoms [6,7].
Aristotle and the philosophy of the heart
Aristotle changed medical philosophy, whereas Hippocrates influenced medical practice. The philosopher approached medicine as a branch of natural philosophy and used the concepts of structure, function, and purpose to describe living things [2,3].
Aristotle developed his cardiocentric physiology in biological treatises such as “Parts of Animals” and “Generation of Animals”, where the heart is presented as the first organ of life, the source of intrinsic heat, and the first structure to form during embryological development. [9]. In “On the Motion of Animals”, the heart is further characterised as the basic origin of movement and vital energy. In these works, the brain is given a secondary, regulatory role, while the heart serves as the primary organ coordinating movement, emotion, and physiological activity. [2,3,9,10]
Aristotelian cardiocentrism was grounded in scientific observation and logical inference. Although subsequent anatomical discoveries modify this hierarchy, the heart's central anatomical position, continual motion, and response to emotional states reinforced its supremacy within his biological paradigm [2,6,9].
Aristotelian causality and medical reasoning
What can be seen as the best of Aristotle’s reasoning in terms of his clinical/medical arguments and definitions are based on his view of the history of organisms. He provided a model for understanding not only how but also why biological facts are obtained on purely clinical grounds, through the use of material, formal, efficient, and final causes [2,3]. In medical contexts, an implication of this causal theory is that it encourages physicians to move beyond mere phenomenology and towards mechanistic explanations. In disease, analyses are employed to investigate underlying structures, therapies, transactions, and operational objectives [2,6,7].
In this respect, cardiocentrism was an ordering principle that permitted the rational comprehension of life, and this Aristotelian tradition is still present within current medical reasoning. Even though their philosophical roots are no longer clearly acknowledged, concepts like pathophysiology, disease processes, and risk-factor analysis are nevertheless based on causal thinking [2,6,7].
Cardiocentrism as a shared foundation
Hippocrates and Aristotle agree on cardiocentrism as a fundamental idea despite variations in methodology. Hippocrates observed that the heart was a critical organ, and if it malfunctioned, disaster for the entire body would soon follow [4,8]. In Aristotle’s case, cardiocentrism emerged less from empirical medicine but rather from Aristotle’s philosophical reflections on the heart as the body’s primary source of motion and life [2,9]. This convergence disqualifies linear medical progress narratives, such as those that “cardiocentrism” was merely some straightforward mistake to be rectified by “neurocentrism.” Rather, cardiocentrism was used as a principle of organisation that guided medical thought over the centuries [6,7]. The focus on the heart remained key to the clinical and symbolic importance of latter models, including those with more emphasis on clinical studies [6,8,11].
From cardiocentrism to modern clinical reasoning
Although the brain’s involvement in cognition and feeling was made clear by advances in anatomy and neuroscience [1,9], the heart's clinical centrality remained intact. Cardiocentrism is still crucial for comprehending circulation, systemic disease, and prognosis, but neurocentrism predominates in explanations of cognition in modern medicine [6,7]. The importance of the heart in determining systemic stability is highlighted by the fact that heart failure, arrhythmias, and circulatory collapse remain crucial thresholds in clinical medicine [6,7]. In this way, cardiocentrism has been reinterpreted within the context of modern biomedical knowledge rather than simply abandoned.
Conclusion
It is best to consider modern medicine as the result of synthesis rather than conflict. While Aristotelian philosophy offered a robust framework for causal explanation and biological comprehension, Hippocratic medicine laid the groundwork for observation, prognosis, and holistic care. A common conceptual basis that still influences modern therapeutic reasoning is cardiocentrism. Although anatomical knowledge has evolved, the heart remains crucial to prognosis, systemic integration, and patient experience. The ongoing value of combining scientific observation, causal reasoning, and meaningful engagement with the patient in a holistic fashion in their entirety is highlighted by the recognition of the cardiocentric roots of medicine.
