



















Keywords
cardio-oncology, cardiotoxicity, chemotherapy, prevention, radiotherapy, risk assessment, targeted therapy
Abbreviation list
ACEI: angiotensin-converting enzyme inhibitors
ARB: angiotensin receptor blockers
CTR-CVT: cancer treatment related cardiovascular toxicity
CV: cardiovascular
CVT: cardiovascular toxicity
EHA: European Haematology Association
ESC: European Society of Cardiology
ESTRO: European Society for Therapeutic Radiology and Oncology
HF: heart failure
HFA: Heart Failure Association of the ESC
ICOS: International Cardio-Oncology Society
LV: left ventricle
LVD: left ventricular dysfunction
LVEF: left ventricular ejection fraction
Take-home messages
- Cardio-Oncology strategies aim at providing optimal cancer therapy while minimising the risk of CTR-CVT.
- The risk of CTR-CVT is a dynamic variable, influenced by several CV and non-CV conditions, that changes during the cancer process.
- Cardio-oncology programmes facilitate a multidisciplinary CVT risk assessment. Baseline CVT risk stratification improves implementation of a personalised surveillance plan.
- Prevention of CTR-CVT remains an important goal for all patients receiving cancer therapy.
- Prescription of lifestyle modifications (diet, exercise) should be part of an integrated approach to CTR-CVT prevention.
- Current pharmacological interventions are recommended for patients at high and very high risk of CTR-CVT.
Impact on practice statement
Baseline CVT risk stratification enables the oncology team to make appropriate cancer treatment choices, educate patients, and define prevention and surveillance strategies. A cardio-oncology referral is recommended (Class I, level of evidence C) for high and very high-risk patients or if CVT develops; it may be considered (Class IIb, level of evidence C) for moderate risk patients.
Patient-oriented message
Some cancer treatments can negatively affect the heart and circulation. The 2022 ESC Guidelines on cardio-oncology provide an overview of the latest recommendations on how these side effects can be prevented, diagnosed, and treated. The 2022 ESC Guidelines describe the factors that increase the risk of cardiovascular toxicity of cancer treatments and contain risk assessment tools which will help to determine the risk profile of every patient and help develop a preventive and monitoring strategy. A lay version of this document will be available soon for patients with cancer, their families, and caregivers. This document should help your patients to understand the importance of making appropriate healthy lifestyle choices and strategies to optimise heart health, during and after cancer treatment.
Introduction
Advances in cancer prevention and treatment have led to a greater number of patients living longer and better lives [1] but, despite these gains, cancer treatment-related CV toxicity (CTR-CVT) is a growing medical problem. This is in part due to the increase in cancer prevalence as well as the complex CV toxicity spectrum of older and newer cancer therapies [2]. The primary goal of cardio-oncology is to allow patients with cancer to receive the best possible cancer treatment safely, while minimising both unnecessary cancer therapy interruptions and CTR-CVT risk [3]. The first European Society of Cardiology (ESC) Guidelines on Cardio-Oncology [4] focuses on the complexity of the interaction between cardiovascular (CV) diseases and cancer to guide clinicians in their daily practice. In this article, we review the proposed strategies to guide CV toxicity (CVT) risk stratification before cancer treatment and CTR-CVT prevention.
Cancer therapy-related cardiovascular toxicity risk stratification
CV toxicity (CVT) risk is a dynamic variable that changes during the cancer process and is influenced by several modifiable and non-modifiable conditions (including age, sex, genetic factors, previous cancer and cancer therapies, and pre-existing CV risk factors and CV diseases) as well as by the type, duration, and intensity of cancer therapies. Therefore, a comprehensive baseline CVT risk assessment is critical to making appropriate cancer treatment choices, organising personalised preventive strategies, and therapy monitoring (Figure 1).
Figure 1. Baseline CV toxicity risk assessment checklist.
Reproduced with permission from [4]: Lyon AR, et al. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Haematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur Heart J. 2022;43:4229-361.
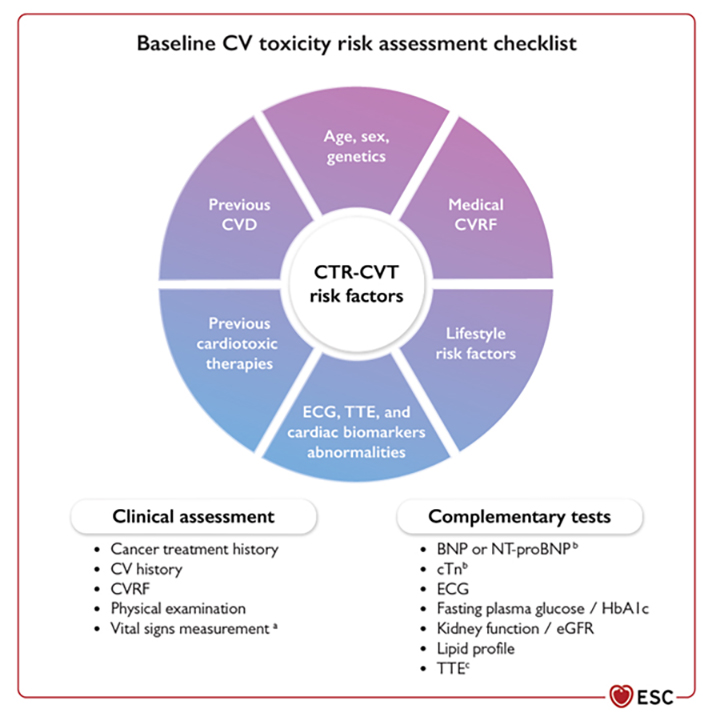
BNP: brain natriuretic peptide; cTn: cardiac troponin; CV: cardiovascular; CVD: cardiovascular disease; CVRF: cardiovascular risk factors; CTR-CVT: cancer treatment-related cardiovascular toxicity; ECG: electrocardiogram; eGFR: estimated glomerular filtration rate; TTE: transthoracic echocardiogram.
Multiple retrospective community-based studies have reported a higher prevalence of conventional CV risk factors among cancer survivors than in the general population and have found that when multiple CVT risk factors co-exist in a patient, they have an additive contribution to the global CVT risk [5]. Consequently, a CVT risk assessment should ideally be performed using a method where all these risk factors are incorporated.
Although prospective validation is needed, the ESC guidelines support the use of the recently developed Heart Failure Association (HFA) and International Cardio-Oncology Society (IC-OS) baseline risk stratification score [6] with a class IIa recommendation, level of evidence C [4]. The HFA-ICOS score was developed, after a systematic analysis of the literature, for seven classes of potentially cardiotoxic cancer therapies (anthracycline chemotherapy, HER2 targeted therapies, vascular endothelial growth factor inhibitors, second and third generation BCR-ABL multi-targeted kinase inhibitors, proteasome inhibitors, RAF and MEK inhibitors, and androgen deprivation therapies for prostate cancer) (Table 1) [4]. To further simplify the use in daily clinical practice, the HFA-ICOS score is available in an interactive format in the ESC Pocket Guidelines App. For patients receiving cancer drugs not included in the HFA-ICOS risk stratification score, new guidelines list the conditions that increase CVT risk (Table 2) [4].
Table 1. Heart Failure Association–International Cardio-Oncology Society baseline cardiovascular toxicity risk stratification.
Reproduced with permission from [4]: Lyon AR, et al. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur Heart J. 2022;43:4229-361.
| Baseline CV toxicity risk factors | Anthracycline chemotherapy | HER2 therapies |
VEGF inhibitors | BCR-ABL inhibitors | Multiple myeloma therapies | RAF-MEK inhibitors |
|---|---|---|---|---|---|---|
| Previous CVD | ||||||
| HF/ cardiomyopathy /CTRCD | VH | VH | VH | H | VH | VH |
| Severe valvular heart disease | H | H | - | - | - | H |
| MI or PCI or CABG | H | H | VH | - | - | H |
| Stable angina | H | H | VH | - | - | H |
| Arterial vascular disease | - | - | VH | VH | VH | - |
| Abnormal ABPI | - | - | - | H | - | - |
| Pulmonary hypertension | - | - | - | H | - | - |
| Arterial thrombosis with TKI | - | - | - | VH | - | - |
| Venous thrombosis (DVT/PE) | - | - | H | M2 | VH | - |
| Arrhythmiaa | - | M2 | M2 | M2 | M2 | M1 |
| QTc ≥480 ms | - | - | H | H | - | - |
| 450 ms ≤ QTc <480 ms (men) 460 ms ≤ QTc <480 ms (women) |
- | - | M2 | M2 | - | - |
| Prior PI CV toxicity | - | - | - | - | VH | - |
| Prior IMID CV toxicity | - | - | - | - | H | - |
| Cardiac Imaging | ||||||
| LVEF <50% | H | H | H | H | H | H |
| LVEF 50–54% | M2 | M2 | M2 | - | M2 | M2 |
| Left ventricular hypertrophy | - | - | - | - | M1 | - |
| Cardiac amyloidosis | - | - | - | - | VH | - |
| Cardiac biomarkers | ||||||
| Elevated baseline cTnb | M1 | M2 | M1 | - | M2 | M2 |
| Elevated baseline NPsb | M1 | M2 | M1 | - | H | M2 |
| Age and CVRF | ||||||
| Age ≥80 years | H | H | - | - | - | H |
| Age 65–79 years | M2 | M2 | - | - | - | M2 |
| Age ≥75 years | - | - | H | H | H | - |
| Age 65–74 years | - | - | M1 | M2 | M1 | - |
| Age ≥60 years | - | - | - | M1 | - | M1 |
| Cardiovascular disease 10-year risk score >20% | - | - | - | H | - | - |
| Hypertensionc | M1 | M1 | H | M1 | M1 | M1 |
| Chronic kidney diseased | M1 | M1 | M1 | M1 | M1 | M1 |
| Proteinuria | - | - | M1 | |||
| Diabetes mellituse | M1 | M1 | M1 | M1 | M1 | M1 |
| Hyperlipidaemiaf | - | - | M1 | M1 | M1 | - |
| Family history of thrombophilia | M1 | M1 | ||||
| Current cancer treatment | ||||||
| Dexamethasone >160 mg/month | - | - | - | M1 | - | |
| Includes anthracycline before HER2-targeted therapy | - | M1g | - | - | - | - |
| Previous exposure to | ||||||
| Anthracycline | H | M2h | H | - | H | H |
| Trastuzumab | - | VH | - | - | - | |
| RT to left chest or mediastinum | H | M2 | M1 | - | M1 | M2 |
| Non-anthracycline chemotherapy | M1 | - | - | - | - | |
| Lifestyle risk factors | ||||||
| Current smoker smoking history | M1 | M1 | M1 | H | M1 | M1 |
| Obesity (BMI >30 kg/m2) | M1 | M1 | M1 | M1 | M1 | M1 |
AF: atrial fibrillation; BCR-ABL: breakpoint cluster region–Abelson oncogene locus; BMI, body mass index; BNP, B-type natriuretic peptide; BP, blood pressure; CABG, coronary artery bypass graft; cTn, cardiac troponin; CTRCD, cancer therapy-related cardiac dysfunction; CV, cardiovascular; CVD, cardiovascular disease; CVRF, cardiovascular risk factors; DM, diabetes mellitus; DVT, deep vein thrombosis; eGFR, estimated glomerular filtration rate; H, high risk; HbA1c, glycated haemoglobin; HER2, human epidermal receptor 2; HF, heart failure; IMiD, immunomodulatory drugs; LV, left ventricular; LVEF, left ventricular ejection fraction; M, moderate risk; MEK, mitogen-activated extracellular signal-regulated kinase; MI, myocardial infarction; MM, multiple myeloma; NP, natriuretic peptides (including BNP and NT-proBNP); NT-proBNP, N-terminal pro-B-type natriuretic peptide; PCI, percutaneous coronary intervention; PE, pulmonary embolism; PH, pulmonary hypertension; PI, proteasome inhibitors; QTc, corrected QT interval; RAF, rapidly accelerated fibrosarcoma; RT, radiotherapy; TKI, tyrosine kinase inhibitors; ULN, upper limit of normal; VEGFi, vascular endothelial growth factor inhibitors; VH, very high risk; VHD, valvular heart disease.
Risk level: Low risk=no risk factors OR one moderate 1 risk factor; moderate risk (M)=moderate risk factors with a total of 2–4 points (Moderate 1 [M1] =1 point; Moderate [M2] =2 points); high risk (H)=moderate risk factors with a total of ≥5 points OR any high-risk factor; very-high risk (VH)=any very-high risk factor.
a AF, atrial flutter, ventricular tachycardia, or ventricular fibrillation.
b Elevated above the ULN of the local laboratory reference range.
c Systolic BP > 140 mmHg or diastolic BP > 90 mmHg, or on treatment.
d eGFR < 60 mL/min/1.73 m2.
e HbA1c > 7.0% or >53 mmol/mol, or on treatment.
f Non-high density lipoprotein cholesterol >3.8 mmol/L (>145 mg/dL) or on treatment.
g High risk if anthracycline chemotherapy and trastuzumab delivered concurrently.
h Previous malignancy (not current treatment protocol).
Table 2. Baseline predictors of high or very high cardiovascular toxicity risk.
| Therapies | Patients at high or very high cardiovascular toxicity risk |
|---|---|
| Bruton tyrosine kinase inhibitors |
|
| Immune check-point inhibitors |
|
| CAR-T and TIL therapies |
|
| Haematopoietic stem cell transplantation |
|
| Radiotherapy |
Very high risk according to MHD received
High risk according to MHD received
|
ASTCT: American Society for Transplantation and Cellular Therapy; Gy: grey; ICI: immune check-point inhibitors; MHD: mean heart dose.
To complete the CVT risk evaluation, an electrocardiogram is recommended in all patients before cardiotoxic therapies (class I, level of evidence C) [4]. Cardio-oncology guidelines have also set precise recommendations for baseline transthoracic echocardiography and cardiac biomarkers assessment according to the type of cancer treatment and the baseline estimated HFA-ICOS risk score.
After completing CVT risk assessment we can establish a precise clinical pathway of care for each patient. Low risk patients should proceed to anticancer therapy without delay (class I, level of evidence C) [4]. In moderate risk patients, a cardio-oncology referral may be considered in selected patients (class IIb, level of evidence C) [4]. A cardiology referral is recommended in high and very-high risk patients before cancer treatment (class I, level of evidence C) and for those with abnormal findings at the baseline CV toxicity risk assessment (either electrocardiogram, cardiac biomarkers, or cardiac imaging) (class I, level of evidence C) [4].
Cancer therapy-related cardiovascular toxicity prevention
Optimisation of cardiovascular health and prevention of CTR-CVT is paramount to offering patients the best possible cancer therapy. The recent ESC guidelines provide recommendations on the determination of CTR-CVT risk (low, moderate, high, or very high) for a variety of anti-cancer therapeutics (e.g., cytotoxic agents, immunotherapies, radiation, and hormone therapies) [4] but for those patients identified to be at high or very high risk, what evidence do we have to support the use of primary prevention strategies?
Anthracyclines remain an important component of anti-cancer therapy for both solid and haematological malignancies; however, they are associated with an increased risk of left ventricular dysfunction (LVD) and heart failure (HF) based on a cumulative dose (>250 mg/m2) and the presence of CV risk factors and/or disease [7]. Several strategies have been recommended to decrease anthracycline related cardiotoxicity including longer infusion times, liposomal formulations and dexrazoxane. Consideration of liposomal anthracyclines in adult patients at high and very high risk of CTR-CVT when anthracycline chemotherapy is indicated is a reasonable approach as recommended by the ESC guidelines (class IIa, level of evidence B) (Figure 2) [4]. Dexrazoxane has been studied as a cardioprotective agent both in the paediatric and adult cancer population for anthracycline induced CTR-CVT [8]. However, it is only approved by the U.S. Food and Drug Administration (FDA) for use in patients with advanced or metastatic breast cancer who have a minimum cumulative dose of 300 mg/m2 or the equivalent [4,7].
The ESC guidelines recommend dexrazoxane infusion in adult patients with cancer scheduled to receive a high total cumulative anthracycline dose for curative treatment, and in patients with high and very high cancer therapy-related cardiac dysfunction (CTRCD) risk, including those with pre-existing HF or low-normal or reduced left ventricular ejection fraction (LVEF) where anthracycline chemotherapy is deemed essential (class IIa, level of evidence B) [4].
Figure 2. Primary and secondary cancer therapy-related cardiovascular toxicity prevention.
Reproduced with permission from [4]: Lyon AR, et al. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur Heart J. 2022;43:4229-361.
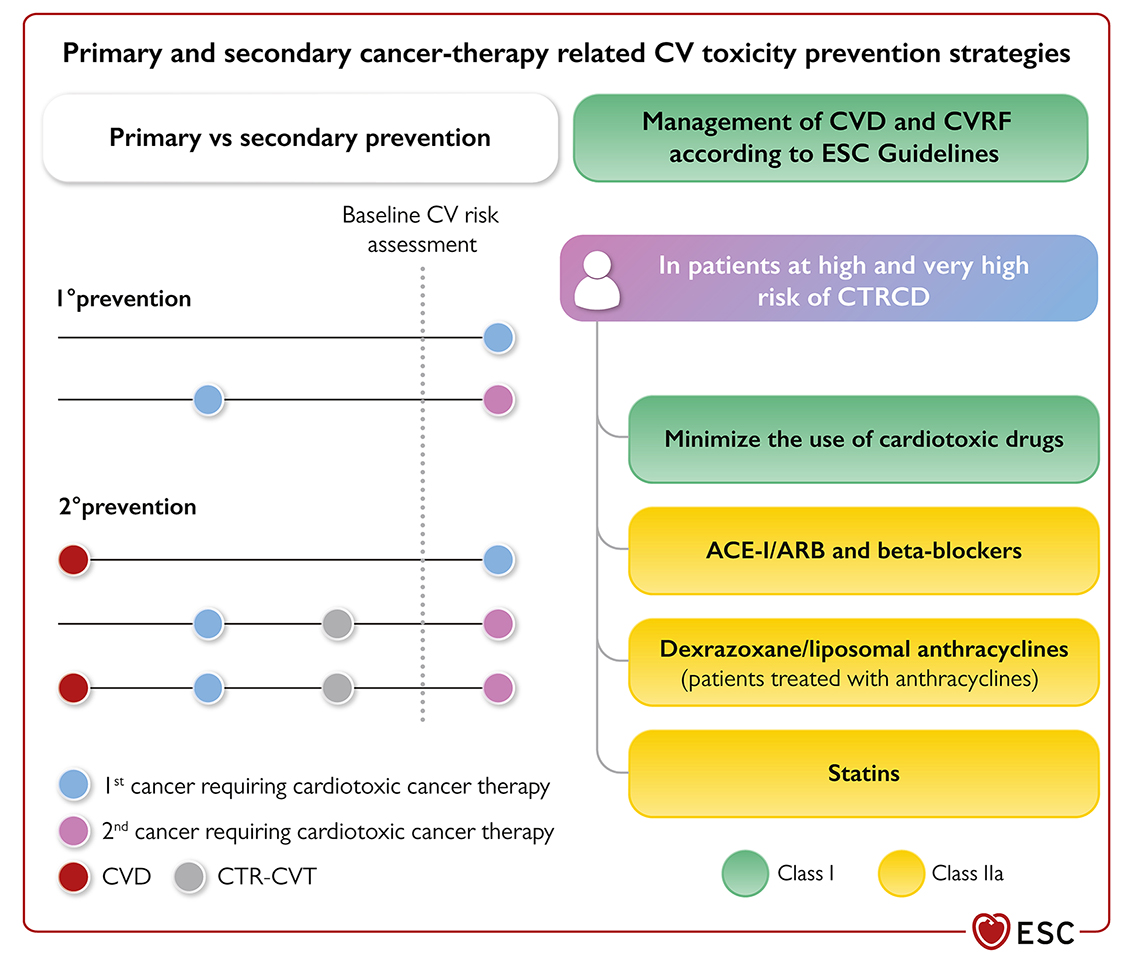
ACE-I: angiotensin-converting enzyme inhibitors; ARB: angiotensin receptor blockers; CV: cardiovascular; CVD: cardiovascular disease; CVRF: cardiovascular risk factors; CTR-CVT: cancer therapy-related cardiovascular toxicity; CTRCD: cancer therapy-related cardiac dysfunction; ESC: European Society of Cardiology.
Several studies have explored the cardioprotective efficacy of neurohormonal strategies with angiotensin inhibitors (ACEI), angiotensin receptor blockers (ARB) and beta blockers, mainly in breast cancer patients receiving anthracycline-containing regimens +/- trastuzumab. In a recent meta-analysis including patients with cancer treated with anthracycline chemotherapy and HER2 targeted therapies, a significant benefit in the use of neurohormonal therapy was seen with the prevention of LVEF reduction. However, there was no statistical difference in the incidence of overt HF or clinical outcomes [9].
Small studies conducted in relatively young, healthy patients (mainly breast cancer) with few comorbidities, different definitions of cardiotoxicity, different cardiac medications, and short duration of follow-up, may account for the small benefits reported in the literature [10]. Based on the literature, the ESC guidelines recommend that ACEIs, ARBs, and beta blockers should be considered for patients receiving anthracyclines and/or anti-HER2 therapies at high and very high CVT risk, (class IIa; level of evidence B) as well as for those receiving other cancer therapies that may cause HF (class IIa; level of evidence C) [4]. Additional large-scale trials are needed before these agents are recommended as a standard of care for lower risk patients exposed to potentially cardiotoxic cancer therapy.
Mineralocorticoid receptor antagonists such as spironolactone, in addition to ACEIs, ARBs or beta blockers, have been shown to reduce CV mortality in HF patients with reduced LVEF. Mineralocorticoid receptor antagonists are currently being explored for the reduction of anthracycline induced cardiotoxicity [11]. Statins are another class of drug being explored for their cardioprotective role in cancer patients exposed to cardiotoxic agents and are currently recommended by the ESC guidelines for primary prevention in patients with cancer at high and very high risk of CTR-CVT (class IIa; level of evidence B) [4].
While the impact of current pharmacological prevention strategies continues to evolve, it is important to consider the benefit of lifestyle modifications. A diagnosis of cancer, particularly in the advanced stages, can lead to depression, sedentary behaviour, loss of functional capacity and weight gain all of which can increase an individual’s risk of experiencing a cardiac event particularly while on active cancer therapy. Studies, mainly in the breast cancer population, have demonstrated fewer cardiovascular events in cancer patients who exercise on a regular basis [12]. The American Heart Association recommends a comprehensive model (CORE) to identify patients at high risk of CTR-CVT and the use of a multimodality approach (exercise plus nutritional counselling and CV risk assessment) to prevent or mitigate cardiovascular events [13].
While the current ESC guidelines recommend cardioprotective strategies be incorporated into treatment plans for those individuals at high and very high risk of CTR-CVT, optimal strategies (i.e. the best drugs and duration of treatment) have yet to be defined. Several on-going studies (PROACT; ICOS-ONE) are investigating the role of enalapril in preventing anthracycline-induced cardiotoxicity. The Southwest Oncology Group (SWOG) S1501 trial is investigating the efficacy of carvedilol vs no intervention in metastatic HER2 + breast cancer patients receiving cardiotoxic cancer therapy and the PRADA II study is evaluating the role of sacubitril/valsartan in attenuation of LVEF decline at 18 months. STOP-CA and PREVENT are both evaluating the efficacy of statins as a primary prevention strategy in patients with non-Hodgkin’s lymphoma and breast cancer. There are several on-going studies evaluating the role of diet and exercise interventions. The CARDAPAC study is exploring the impact of individualised exercise interventions in breast cancer patients treated with trastuzumab on metabolic and hormonal responses including LVEF [10].
Prevention of CTR-CVT remains an important goal for all patients receiving cancer therapy. Liposomal doxorubicin, dexrazoxane, statins and neurohormonal strategies are currently recommended by the ESC for those patients at high and very high risk (Figure 2). However, further studies are needed to determine the best drugs, efficacy, optimal duration, and dose of pharmacological interventions in broader (non-breast) cancer populations. Prescription of lifestyle modifications (diet, exercise) should be part of an integrated approach to prevention strategies in this patient population. Our goal as clinicians should be to provide optimal cancer therapy while minimising any potential detrimental impact on CV health.