

















Keywords
sleep apnoea, cardiovascular disease, CPAP therapy, diagnostic pathways
Abbreviation list
AF: atrial fibrillation
CPAP: continuous positive airway pressure
CSA: central sleep apnoea
HFrEF: heart failure with reduced ejection fraction
OSA: obstructive sleep apnoea
Patient-oriented messages
Sleep apnoea is a common condition where breathing repeatedly stops during sleep. While it's often linked to feeling tired during the day, many people with heart conditions have sleep apnoea without feeling tired at all. Sleep apnoea can quietly increase the risk of high blood pressure, irregular heart rhythms, heart failure, and stroke. If you have a heart condition — especially if you snore, wake up at night gasping, have daytime sleepiness or hard-to-control blood pressure — it’s worth discussing sleep apnoea with your doctor. Simple home tests and effective treatments are available and may help protect your heart and overall well-being.
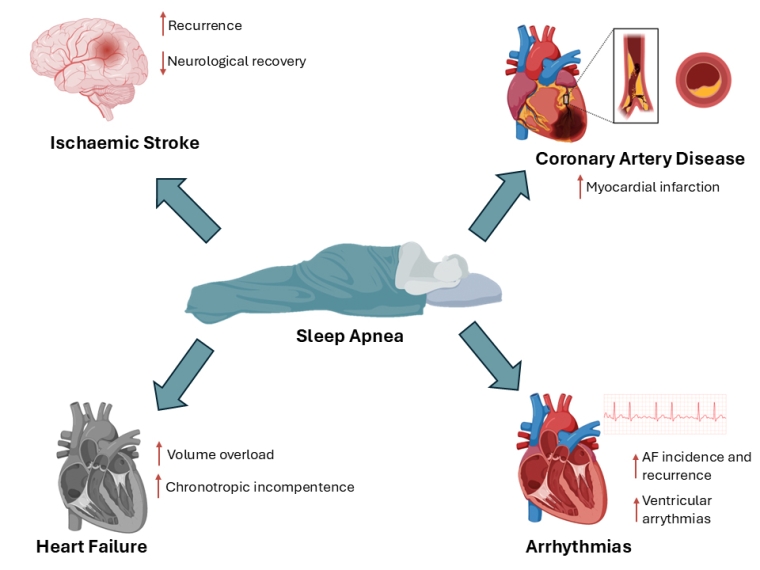
Central illustration. Sleep apnoea and its impact on cardiovascular risk.
Introduction
Sleep apnoea is a common, yet frequently underdiagnosed, sleep-related breathing disorder characterised by recurrent episodes of apnoea (complete cessation of airflow) or hypopnoea (partial airflow reduction) during sleep. These events lead to intermittent hypoxia, arousals, and sympathetic activation, with downstream effects on cardiovascular, metabolic, and neurocognitive health.
Two main types of sleep apnoea exist: obstructive sleep apnoea (OSA), caused by recurrent upper airway collapse despite ongoing respiratory effort, and central sleep apnoea (CSA), due to reduced central respiratory drive. OSA is more common and associated with obesity and anatomical factors, while CSA is typically seen in patients with heart failure and in opioid use.
OSA affects an estimated 10-20% of the general population, with higher rates in men and individuals with obesity. Among patients with cardiovascular disease, prevalence is much higher, with up to 50% having undiagnosed OSA. CSA is less common but occurs in 30-50% of patients with heart failure with reduced ejection fraction (HFrEF), especially with Cheyne-Stokes respiration.
Sleep apnoea contributes to increased healthcare use, hospitalisations, and cardiovascular risk, including hypertension, ischaemic stroke, myocardial infarction, and arrhythmias. In Europe, the economic burden is estimated in the billions annually [1].
Why cardiologists should care
Sleep apnoea — particularly OSA — is highly prevalent in patients with cardiovascular disease, affecting up to 50% of those with HT, coronary artery disease (CAD), atrial fibrillation (AF), and as many as 80% of patients with heart failure [2-5]. Both OSA and CSA contribute to disease progression through mechanisms such as sympathetic activation, oxidative stress, systemic inflammation, and blood pressure variability.
Sleep apnoea is independently associated with increased risk of incident and recurrent AF, resistant hypertension, ischaemic stroke, heart failure exacerbation, and mortality. Importantly, it may also reduce the effectiveness of cardiovascular therapies, including catheter ablation, cardiac resynchronisation therapy, and pharmacological interventions.
Given the strong bidirectional relationship between sleep apnoea and cardiac disease, cardiologists are uniquely positioned to identify and refer at-risk patients. Recognition and appropriate management may improve cardiovascular outcomes, reduce hospitalisations, and improve quality of life for patients with cardiovascular diseases.
Pathophysiology: the cardiovascular connection
Sleep apnoea exerts harmful cardiovascular effects through both acute and chronic physiological pathways, many of which are highly relevant to cardiologists.
Acute effects
Each apnoeic episode leads to intermittent hypoxia and hypercapnia, triggering sympathetic nervous system activation. Negative intrathoracic pressure swings increase cardiac afterload and impair venous return, especially in heart failure. These events cause transient surges in blood pressure and heart rate, contributing to arrhythmogenesis and nocturnal hypertension [6].
Chronic consequences
Over time, repetitive stress from sleep apnoea promotes systemic inflammation, oxidative stress, and endothelial dysfunction. These mechanisms accelerate atherosclerosis, worsen insulin resistance, and contribute to metabolic syndrome. The cumulative burden increases the risk of sustained hypertension, CAD, heart failure, and AF [6].
Cardiovascular impact of sleep apnoea
Sleep apnoea and cardiovascular diseases share many common risk factors, including obesity, advancing age, male sex, and metabolic dysfunction. Beyond this overlap, sleep apnoea also contributes directly to the development and progression of cardiovascular disease through distinct pathophysiological mechanisms.
Hypertension
Sleep apnoea is a well-established contributor to resistant hypertension and is associated with nocturnal hypertension patterns due to nocturnal sympathetic surges. Repetitive apnoeic events blunt the normal nocturnal blood pressure fall, contributing to increased cardiovascular risk [6].
Coronary artery disease (CAD)
OSA increases the risk of myocardial infarction and is associated with plaque instability through systemic inflammation, oxidative stress, and blood pressure variability. Perioperatively, undiagnosed OSA may increase the risk of adverse cardiac events, highlighting the need for preoperative screening in patients undergoing cardiac surgery [6].
Heart failure
In HFrEF, both OSA and CSA are common and prognostically significant. CSA, particularly with Cheyne-Stokes respiration, is linked to increased mortality. Importantly, the pivotal SERVE-HF trial surprisingly showed that adaptive servo-ventilation (i.e., a device that adjusts pressure support breath-by-breath to stabilise breathing patterns) in patients with CSA and HFrEF may increase cardiovascular mortality and should be avoided in this population [7].
In HFpEF, OSA is prevalent and contributes to volume overload, diastolic dysfunction, and chronotropic incompetence. Recognition and treatment of sleep apnoea in HF may improve symptoms, quality of life, and functional capacity.
Arrhythmias
Sleep apnoea is strongly associated with AF, both incident and recurrent. It promotes arrhythmogenesis via autonomic imbalance, atrial stretch, and inflammation. OSA reduces the success of AF catheter ablation and increases recurrence risk if left untreated. It is also linked to ventricular arrhythmias and sudden cardiac death, particularly during sleep [8].
Ischaemic stroke
OSA is an independent risk factor for ischaemic stroke and is frequently present in the post-stroke period. It may impair neurological recovery and increase risk of recurrent stroke. Screening for sleep apnoea in stroke patients is underutilised but may offer therapeutic and rehabilitative benefits.
Screening tools for sleep apnoea
Symptoms of OSAS are detailed in the article by Drs Gervasio and Moglio which also is published in the series on CardioPractice.
Several screening questionnaires have been developed to identify patients at risk of sleep apnoea, including:
- STOP-BANG: Incorporates snoring, tiredness, observed apnoeas, high blood pressure, BMI, age, neck circumference, and gender.
- Epworth Sleepiness Scale: Assesses daytime sleepiness based on the likelihood of dosing in various situations.
- Berlin Questionnaire: Stratifies risk based on snoring severity, daytime fatigue, and comorbidities.
While these tools are widely used in sleep medicine, they have limited sensitivity and specificity in cardiac populations. Many cardiovascular patients — particularly those with AF or HF — do not report classic symptoms such as excessive daytime sleepiness, leading to false-negative results [9,10].
Nevertheless, these tools can help raise awareness among cardiologists by highlighting key symptoms and risk factors of sleep apnoea. While not sufficiently accurate for diagnosis, they can serve as a clinical prompt to consider sleep apnoea in patients with cardiovascular diseases. Currently, the value of using these tools for screening purposes in patients with cardiac conditions is undetermined. Recognising the broader spectrum of symptoms — such as nocturnal choking, gasping, or unexplained fatigue — may help cardiologists identify patients who would benefit from further evaluation.
Diagnostic approach
When to refer for a sleep study
Cardiologists should consider referral for sleep testing in patients with resistant hypertension, recurrent heart failure decompensations, difficult-to-control AF, or nocturnal symptoms such as gasping, choking, or frequent awakenings. These clinical red flags may suggest underlying sleep apnoea, even in the absence of daytime sleepiness. Referral should be considered when sleep apnoea may be contributing to cardiovascular instability (e.g., worsening HF, arrhythmia burden).
Types of sleep studies
In-laboratory polysomnography remains the gold standard for diagnosing sleep apnoea whose technique is discussed in detail in the article by Drs Gervasio and Moglio (LINK TO BE ADDED HERE). Especially in patients with complex comorbidities, suspected CSA, or when previous home-based testing has been inconclusive, in-laboratory polysomnography is essential. However, it is often cumbersome, time-consuming, and resource-intensive, which can limit accessibility. Home sleep apnoea testing (HSAT), on the other hand, is increasingly accessible and cost-effective. Emerging HSAT systems such as WatchPAT ONE, SleepImage, and NightOwl offer cardiologists new pathways to screen patients remotely. These devices use surrogate markers (e.g., peripheral arterial tone, heart rate variability, oxygen desaturation indices) and are being integrated into decentralised care models, expanding access while maintaining diagnostic yield.
Sleep study interpretation focuses on a few key parameters. The Apnoea-Hypopnoea Index (AHI) quantifies event frequency per hour, with values ≥5 indicating sleep apnoea and ≥15 typically prompting treatment. Oxygen desaturation patterns provide insight into severity — intermittent drops are characteristic of OSA, while sustained or cyclic desaturations may indicate CSA.
Recently, the Apple Watch also includes a feature called “Breathing Disturbances” which, over a 30-day period of nightly wear based on accelerometer data, highlights for potential sleep apnoea [11]. Nevertheless, the clinical effect of consumer-aimed wearable devices has yet to be determined.
Local causes of OSAS may require an otolaryngology study which is detailed in the article by Drs. Gervasio and Moglio.
Treatment options and cardiovascular benefits
Continuous positive airway pressure (CPAP)
CPAP remains the first-line treatment for moderate-to-severe OSA in patients with cardiovascular diseases. It prevents upper airway collapse by maintaining positive airway pressure throughout the respiratory cycle.
CPAP has been shown to modestly lower blood pressure, with average reductions of 2-4 mmHg in overall populations and up to 7-10 mmHg in patients with resistant hypertension, where sympathetic overactivity and nocturnal blood pressure surges are particularly pronounced. These effects may be more pronounced with good adherence (≥4 hours per night) and in patients with severe OSA [12].
Furthermore, CPAP may help reduce the risk of AF recurrence, particularly in patients undergoing catheter ablation. Observational studies and meta-analyses have shown that OSA treatment is associated with up to a 42% reduction in AF recurrence following ablation, likely by reducing atrial remodelling, autonomic imbalance, and inflammation. However, randomised data are still limited, and ongoing trials aim to clarify the extent of benefit [13].
Importantly, CPAP is not suitable for all cardiac patients. In the SERVE-HF trial, ASV was associated with increased cardiovascular mortality in patients with HFrEF and predominant CSA, and CPAP is thus contraindicated in this subgroup.
Adherence remains a major challenge of CPAP treatment, particularly among asymptomatic or minimally symptomatic patients with cardiovascular diseases who may not perceive potential longer-term benefits. Education, close follow-up, and behavioural support are essential to improve long-term compliance.
Alternative therapies
While alternative therapies are rarely used as first-line treatments in patients with cardiovascular diseases, they may be appropriate in selected patients who are CPAP-intolerant or have milder OSA. Mandibular and oral devices, as well as surgical options, are detailed in the Gervasio and Moglio article. Finally, weight management remains a key intervention, with even modest reductions in body weight leading to meaningful improvements in OSA severity, symptoms, and overall cardiovascular risk [14].
Emerging therapies
Hypoglossal nerve stimulation (HGNS) therapy has been suggested as a therapy for lowering systolic blood pressure in patients with moderate-to-severe OSA. However, a recent sham-controlled, randomised crossover therapy trial demonstrated no significant difference between sham and active HGNS therapy in mean 24-hour systolic blood pressure and in sympathetic and vascular measures [15].
In the recent NEJM publication from the SURMOUNT-OSA trials, tirzepatide significantly reduced the AHI by 58–63% in patients with moderate-to-severe OSA and obesity. The beneficial effect appeared to be primarily mediated by substantial weight loss, with additional improvements in oxygenation and inflammatory markers [16]. While promising, the long-term cardiovascular safety and role in non-obese patients remain to be clarified.
Current evidence and future directions
Recent clinical trials
Large-scale trials evaluating the cardiovascular impact of sleep apnoea treatment have yielded mixed results. The SAVE trial, which randomised over 2,700 patients with moderate-to-severe OSA and established cardiovascular disease to CPAP or usual care, found no reduction in major adverse cardiovascular events over a mean of 3.7 years. However, adherence was suboptimal (average ~3.3 hours/night of CPAP), and CPAP did improve sleepiness, quality of life, and mood, underscoring the importance of treatment adherence in interpreting cardiovascular endpoints.
The ADVENT-HF trial assessed the use of ASV in patients with HFrEF. It did not demonstrate a cardiovascular benefit, aligning with concerns previously raised in the SERVE-HF trial. These findings further questioned the role of airway pressure therapies in managing central sleep apnoea in patients with advanced heart failure.
Ongoing research and knowledge gaps
Many questions remain unanswered. There is a lack of clarity around the optimal AHI threshold at which cardiovascular benefits of OSA therapy emerge. Importantly, patient selection remains a key challenge — not all individuals with OSA derive equal benefit from treatment. Targeting those with a high symptom burden, resistant hypertension, arrhythmias, or elevated hypoxic burden may help identify patients more likely to benefit.
Future research should place greater emphasis on patient-reported outcome measures — such as quality of life, fatigue, and daytime functioning — which may more accurately capture meaningful benefits for patients than traditional cardiovascular endpoints alone. As seen in trials like SAVE, even in the absence of reduced event rates, CPAP can lead to significant improvements in symptoms and wellbeing, underscoring the importance of broadening success criteria beyond mortality and hospitalisation.
Future directions
Future directions include personalised medicine approaches that integrate clinical, physiological, and biomarker data to identify patients most likely to benefit from intervention. Emerging biomarkers of hypoxic stress, autonomic dysregulation, or atrial remodelling may help refine treatment thresholds and guide targeted therapy. In parallel, technology integration — including wearable sensors, cloud-based diagnostics, and AI-assisted interpretation — holds promise for earlier detection, remote monitoring, and improved adherence support. As these tools become more accessible, there is growing potential for cardiologists to take primary responsibility for identifying and initiating workup for sleep apnoea in high-risk cardiovascular patients, embedding diagnostics within routine cardiology care pathways to reduce underdiagnosis and streamline management.
Impact on practice statement
Sleep apnoea is highly prevalent among patients with cardiovascular diseases and contributes to hypertension, arrhythmias, heart failure, and ischaemic stroke. Cardiologists should maintain a high index of suspicion for sleep apnoea, particularly in patients with resistant hypertension, AF, or recurrent heart failure deterioration. Although traditional screening tools have limitations, emerging home-based diagnostic methods present new opportunities for timely detection. Implementing structured screening protocols, developing referral pathways, and adopting collaborative care models may improve diagnosis and treatment rates. As the evidence base expands, cardiology-led approaches to identifying and managing sleep apnoea should be integrated into routine cardiovascular care to improve patient outcomes.