




















Keywords
isolated tricuspid regurgitation; echocardiography
Abbreviations
TR tricuspid regurgitation
TV tricuspid valve
AF atrial fibrillation
RV right ventricle
TTE transthoracic echocardiography
Take-home messages
- TR is a major public health problem, as prevalent as aortic stenosis, with the elderly population having a higher incidence of TR compared to other age groups. When TR is present without significant coexisting left ventricular dysfunction or left-sided valvular disease, such as mitral or aortic valve disease, it is called isolated TR.
- Severe isolated TR is associated with an increased risk of cardiac events and mortality, independent of other comorbidities or risk factors, while isolated tricuspid valve (TV) surgery is linked to high in-hospital mortality rates due to delayed referral of TR patients.
- The delay in referring TR patients for surgery is mainly due to its non-specific clinical presentation. This, combined with the high mortality rate of isolated TR surgery, has led to the development of tricuspid transcatheter interventions (TTVI).
- Not all patients with TR are suitable for TTVI. A holistic patient evaluation is necessary when choosing the best candidate for TTVI. This involves (i) a comprehensive assessment of the patient's clinical status, comorbidities, and fraility status; (ii) assessment of TR severity following optimization of loading conditions by diuretic therapy and after implementation of rhythm/rate control strategies in atrial fibrillation patients; (iii) meticulous evaluation of TR phenotype, predominant mechanism(s), and functional anatomy.
- It is essential for clinicians to remember that diuretics do not treat the underlying cause of congestion. It is crucial to closely monitor patients with significant TR with serial clinical and echocardiographic examinations to ensure that surgical or interventional correction is performed before significant RV dysfunction and other organ damage develop. [Identification of isolated TR patients at risk]
Patient-oriented message
TR is a common and serious medical condition that can cause an increase in mortality and a decrease in the quality of life. However, the negative outcomes of TR can be prevented with proper awareness of its symptoms, screening with echocardiography for an accurate and timely diagnosis, close follow-up with echocardiographic reassessment in case of significant TR, and timely interventional or surgical correction.
Impact on practice statement
Recently, there has been a growing interest in tricuspid regurgitation (TR) due to its high prevalence and negative impact on patient health and survival. This can be largely explained by the advancements in the diagnostic and therapeutic approaches to significant TR. Firstly, three-dimensional echocardiography enables better visualisation of the tricuspid valve’s complex anatomy and a better evaluation of TR severity, improving diagnostic accuracy and enabling better risk stratification. Secondly, tricuspid transcatheter intervention (TTVI) has emerged as an appealing alternative for patients with significant isolated TR at high risk for classic surgical intervention, with echocardiography playing an essential role in patient selection and guiding this intervention. However, as not all TV morphologies are suitable for TTVI, proper selection of candidates is necessary, incorporating both clinical and imaging information.
Introduction
Tricuspid regurgitation (TR) is an important public health problem associated with significant symptomatic burden and high mortality. Clinically relevant (moderate or greater) TR is common in the general population (0.55%), increasing in prevalence with aging, particularly in women, who are more affected than men. Elderly people have very high absolute rates of TR, with 1 in 25 people aged 75 and older having moderate or severe TR. Compared to left-sided valve disease, all-cause TR is as prevalent as aortic stenosis [1]. More than 90% of clinically relevant TR cases are functional or secondary (STR).
Secondary TR (STR) is not a disease of the tricuspid valve (TV) itself, as the leaflets are structurally intact; it is rather the result of various diseases (pulmonary hypertension, left-sided valve diseases, cardiomyopathies, or atrial fibrillation [AF], etc) that cause right chamber remodeling, which in turn promotes progressive annular dilatation, leaflet tethering, and their malcoaptation.
On the other hand, primary TR is the result of a direct injury to the TV leaflets, often due to congenital anomalies (i.e., Ebstein), rheumatic heart disease, endocarditis, tumours (i.e., carcinoid syndrome), trauma, or radiation. A distinct category, labeled cardiovascular implantable electronic device (CIED)-induced TR, has emerged, encompassing cases of direct valve injury from a permanent pacemaker or implantable cardioverter-defibrillator lead placement or removal (Type A CIED-related TR), and cases in whom the TR evolves due to the remodelling of the RV induced by the pacing rhythm (Type B CIED-related TR).
What is meant by “isolated” tricuspid regurgitation?
For many clinicians, isolated TR means that the main problem is confined to the TV without significant involvement of the other valves. In past literature, the term “isolated TR” has been inconsistently assigned to TR occurring due to different underlying causes, including an isolated primary disease of TV leaflets, a device (pacemaker or implantable cardiac defibrillator) impinging on a leaflet, to lone AF, to STR progression after left-sided valve surgery or, on the contrary, to STR occurring in patients without left-sided surgery [2-5]. Despite being viewed as leading to the same disease, it became evident that these conditions evolving with isolated TR demonstrate distinct pathophysiological mechanisms, as well as different underlying remodeling of the TV apparatus and right heart chambers, outcomes, and surgical risk.
Later on, isolated TR emerged as a diagnosis of exclusion of other potential known aetiologies of TR (i.e., “unexplained” TR) and was restricted to patients without significant pulmonary hypertension or left-sided diseases and no organic, congenital, or CIED-related involvement of the leaflets [1]. It soon became evident that patients with no apparent cause for isolated TR shared some common features: elderly patients, more commonly women, the vast majority having atrial arrhythmias (AF or flutter) and/or heart failure with preserved ejection fraction (HFpEF), a dilated right atrium (RA) and tricuspid annulus and preserved left (LV) and right ventricular (RV) function. These patients represent a distinct subgroup of STR, classified as “atrial STR” (A-STR) [6]. The recent Tricuspid Valve Academic Research Consortium (TVARC) document recommended to use the term A-STR for any STR in which atrial/annular dilatation is the main mechanism of regurgitation and separately classify it from the more prevalent form of STR in which RV dilatation/dysfunction is the main mechanism of regurgitation (ventricular STR, V-STR) [7].
Isolated tricuspid regurgitation outcomes and treatment
Left untreated, severe isolated TR significantly worsens survival. Data from the European Society of Cardiology (ESC) Heart Failure Long-Term Registry showed that isolated TR was associated with an unexpectedly poor outcome, and HFpEF was one of the main drivers of isolated TR [8]. Notably, severe isolated TR is linked to an excess in cardiac events and mortality, independently of cardiac rhythm or other cardiovascular or comorbid conditions [9]. Moreover, AF patients with clinically relevant isolated TR exhibit not only increased RA dimensions and conical RV remodelling but also higher rates of mortality, heart failure hospitalisations, and stroke when compared to patients without significant isolated TR [10].
Historically, isolated standalone TV surgery has been associated with high in-hospital mortality rates (10%), largely due to the late referral of TR patients [4]. Indeed, most patients with severe isolated TR are referred too late for surgical intervention, when the disease has already advanced to significant RV dilation and dysfunction, right heart failure, and severe kidney and liver insufficiency. The severity of the clinical presentation before surgery has a greater impact on patient outcome than the TR mechanism/aetiology. When surgery is performed early, results are optimal and valve repair is generally possible, underlining that these patients should be identified and referred in a timely manner, before TR-mediated organ damage ensues [11]. Conversely, patients with advanced RV dysfunction do not benefit significantly from valve repair or replacement [6].
The high risk of isolated TR surgery has led to these patients being largely undertreated by cardiac surgery, but also to the rapid development of tricuspid transcatheter interventions (TTVI). TTVI has emerged as a promising therapeutic option, especially for patients with moderate to severe or severe TR deemed inoperable or at high risk for open-heart surgery due to comorbidities, advanced age or prior cardiac interventions. Inspired by the success of transcatheter mitral interventions, similar minimally invasive interventions for TV have been developed. However, the TV anatomy and the pathophysiology of TR are more complex than that of the mitral valve, and while TTVI can improve the quality of life, its effects on the overall survival rates are debatable. Therefore, before deciding on TTVI, it is essential to ensure that the benefits outweigh the procedural risks.
Identification of the best candidates for TTVI requires a greater level of detail in the clinical and anatomic characterisation of this highly heterogeneous group of patients, and identification of patient clusters among those with isolated TR that derive the most benefit from a certain type of treatment is mandatory. As not all TVs are suitable for TTVI, proper evaluation and characterisation of the anatomy with transthoracic and transoesophageal echocardiography, computed tomography, and cardiac magnetic resonance imaging is needed. Patients with unfavourable TTVI anatomy include those with large coaptation gap (>8.5 mm), leaflet thickening and shortening due to rheumatic or carcinoid changes, marked tethering, leaflet perforation, anteroposterior jet origin of the TR, or CIED-related TR [6].
The clinical presentation of isolated TR is variable and based on its severity and impact on RV systolic performance. Patients with TR are highly symptomatic, but most frequently, patients’ symptoms are unspecific, and significant TR is not necessarily suspected during clinical examination, as cardiac auscultation is rarely typical or reliable. Signs and symptoms such as fatigue, dyspnoea, peripheral oedema, ascites, hepatic congestion, and jugular venous distension are usually ascribed to advanced age and not to TR, and because of this, significant TR remains often underdiagnosed and undertreated. It is important to know that as the number of symptoms and signs of congestion increases, so does the mortality rate for significant TR [12].
Given the non-specific clinical presentation in routine clinical practice, a reliable diagnosis of significant TR usually relies on transthoracic two-dimensional (2D) Doppler echocardiography. Importantly, TR severity may vary significantly from one echo exam to another due to RV plasticity, different loading conditions, and the start of diuretic therapy. The TR severity should be reassessed after the optimisation of the loading conditions before referring the patient to any type of invasive treatment [6]. Invasive treatment in symptomatic subjects with isolated TR is recommended to be performed early, before they present recurrent hospitalisations for intractable heart failure, with significant oedema, ascites, and liver dysfunction. However, all physicians should be aware of the fact that, while diuretics can be efficient in controlling symptoms and congestion related to TR, these drugs do not correct the underlying mechanism of TR. Long-term treatment with high-dose diuretics without interventional or surgical correction of TR eventually leads to end-stage heart failure and irreversible organ damage (i.e., advanced chronic kidney and liver diseases).
A routine transthoracic echocardiography (TTE) can provide valuable insights into the pathophysiology of isolated STR. As opposed to V-STR due to pulmonary hypertension when the RV becomes more elliptical, leading to the tethering of TV leaflets, A-STR is characterised by the predominant dilation of the tricuspid annulus, RA, and RV basal inflow, leading to exhaustion of the reserve of valvular coverage of the annulus with absent/minimal leaflet tethering [13].
Rhythm control by cardioversion, anti-arrhythmic drugs, and/or cardiac ablation in AF patients should be considered whenever possible in patients with A-STR since successful restoration of sinus rhythm may significantly reduce the severity of TR by promoting reverse remodelling of RA chamber and TV annulus [14].
TTE represents the gold standard imaging technique not only for the diagnosis of TR and assessment of the aetiology, but also for evaluating isolated TR severity.
Qualitative evaluation of TR severity based on a single-plane evaluation of the jet area is misleading and prone to underestimation [15]. An optimal echocardiographic study should include the full range of semi-quantitative and quantitative parameters of TR severity recommended by current guidelines. An effective regurgitant orifice area >40 mm2, and a regurgitant volume greater than 45 mL assessed with the proximal isovelocity surface area typically indicate severe TR [16]. The measurement of the inferior vena cava diameter and its collapsibility with inspiration provides an estimate of RA pressure, which, added to the RV-RA pressure gradient obtained from the Bernoulli equation applied to the TR jet, provides an estimation of pulmonary artery systolic pressure (PASP). However, the echo-Doppler estimate of PASP may be misleading in severe STR (i.e. significant underestimation of PASP), and right heart cardiac catheterisation is mandatory to exclude significant precapillary pulmonary hypertension.
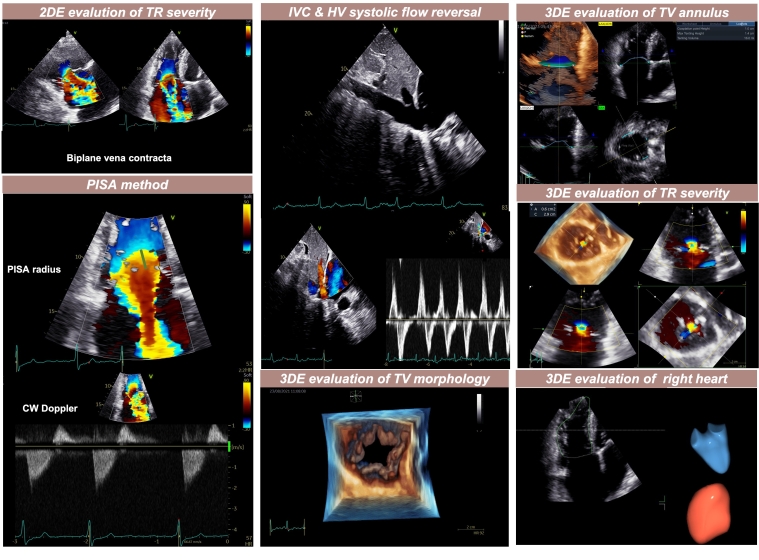
Advanced quantification of RV and RA volumes and function (three-dimensional [3D] echocardiography to assess ejection fraction, and myocardial deformation by speckle-tracking echocardiography to measure longitudinal strain) should be obtained and reported, whenever possible since conventional 2D indices have known limitations in assessing STR. Therefore, it is recommended to include both 3D and speckle-tracking echocardiography in the standard evaluation protocol of patients with TR. This will allow for a more thorough evaluation of the TV’s complex morphology, including the number of leaflets, as well as for a better assessment of the severity of TR through the 3D vena contracta area, and of the impact of TR on right heart chambers (Central Figure).
Central illustration. Integrative assessment of tricuspid regurgitation with two- and three-dimensional echocardiography.
When TTE is inadequate or doubtful, transoesophageal echocardiography and cardiac magnetic resonance should be indicated to clarify the severity and the mechanism of isolated TR. In patients with at least moderate TR, a systematic evaluation of TR severity and mechanism should ideally be done in heart valve clinics with great experience in diagnosing and/or treating TR patients, particularly if the patient belongs to the most challenging patient subsets (e.g., suboptimal acoustic window, previous cardiac surgery, multiple valve diseases, AF, etc). Once the optimal timing of intervention is outlined and the patient is deemed suitable for valve repair/replacement, referral to an expert heart valve hub centre with expertise in surgical and interventional treatment options should be done promptly.
Finally, moderate STR is not benign [17]. This diagnosis should not reassure the doctor nor the patient, particularly if the patient is old, has elevated LV filling pressures/HFpEF, and is in permanent AF [18]. AF is one of the most powerful factors accelerating the progression to severe STR. Some patients with “moderate STR” will actually have severe STR when an accurate imaging assessment is performed. Applying the same severity criteria to A-STR with normal RV size and function and to V-STR with dilated and dysfunctional RV does not appear reasonable. Future studies are needed to refine the assessment of TR severity based on TR phenotype.
A significant TR with an apparently “good” RV, i.e., not significantly dilated or dysfunctional, should not be considered as a sign that the patient can be dismissed with medical treatment and reassured that he/she is well; conversely, close follow-up with a quantitative echocardiography examination every 6-8 months should be recommended to avoid that the optimal window for surgery/TTVI is missed. Subjects with deteriorating RV function, but not end-stage RV failure, should be considered for TR correction.
Conclusion
Even though isolated TR is often under-recognised and undertreated when compared to other valvular heart diseases, it is highly prevalent in the community and associated with increased mortality. However, because of an indistinct clinical presentation, it is necessary to maintain a high level of clinical suspicion. The evolving landscape of diagnostic imaging techniques and percutaneous interventions offers promise and also emphasises the importance of regular screening in high-risk populations. In isolated TR, timely recognition and management are paramount to optimising outcomes, improving life quality, reducing hospitalisations, and lessening the economic burden on the healthcare system.