
Patient
- Woman
- 59 years old
- Obese
- Diabetes
- Hypertension
- Anxiety
- On medication with ramipril, metformine, aspirin 100mg
History
- Husband died two days before from COVID-19
- Fever in the morning
- Admitted to the ER for acute dyspnea, chest pain and agitation
Physical examination
- Pale, sweat, anxious, tachypneic
- BP 195/125, HR 157bpm, SO2 92% room air, t 38°C, RR40
- ABG in VM 40%: pH 7,20, pCO2 34, pO2 73, HCO3 14, lactates 59mg%, glycemia 487mg%
- P/F 180
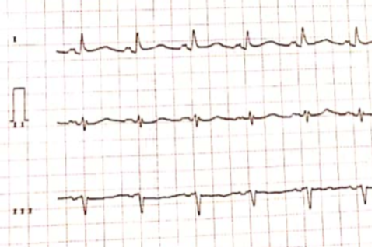
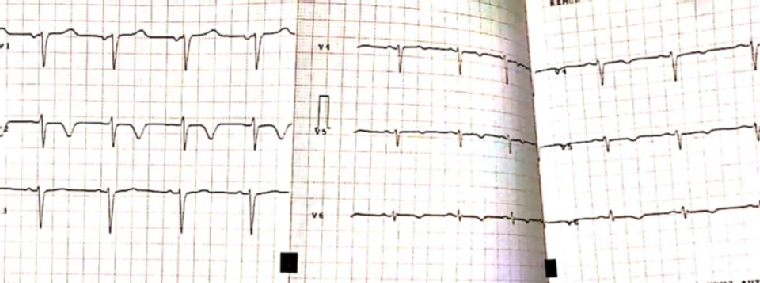
ECG
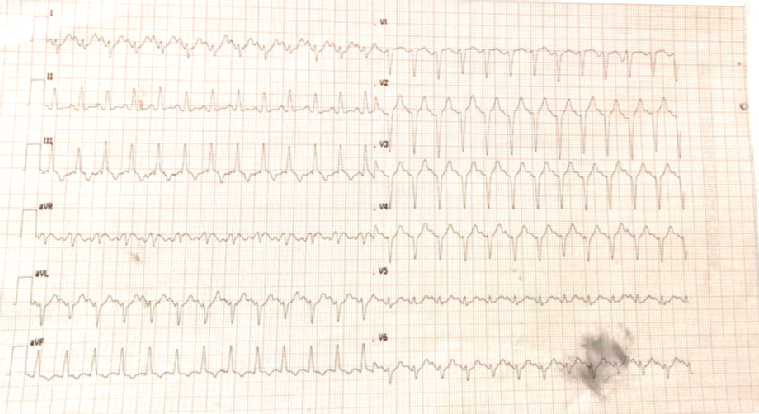
Sinus Tachycardia, negative T waves on AvF an DIII.
No specific alterations of ventricular repolarisation, probably due to hypoxia and respiratory distress.
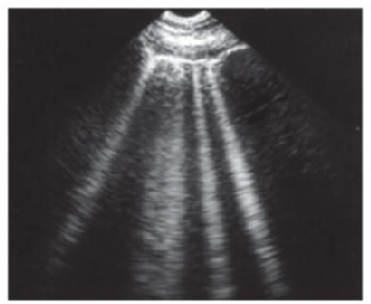
Lung ultrasound

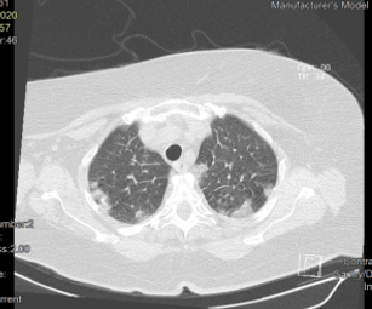
CT scan
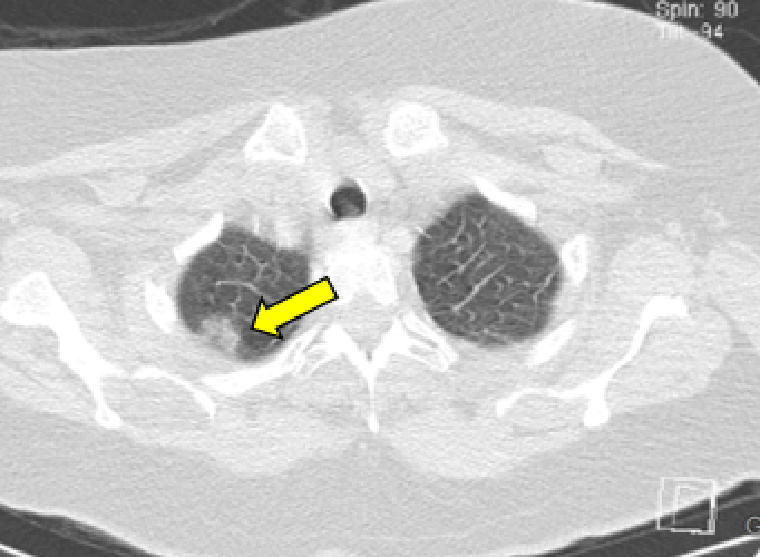
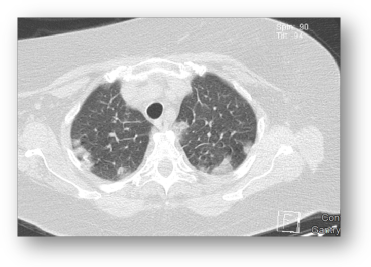
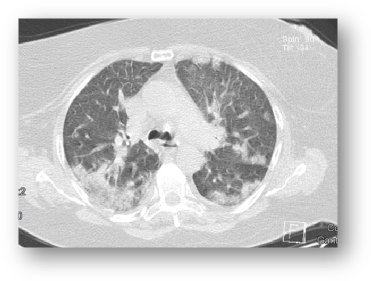
HRCT images showing multifocal and bilateral parenchymal opacities with predominant ground-glass (yellow arrow) associated with the consolidative component (white arrow).
- Multiple ground-glass opacities
- Pulmonary consolidation

Lab exam
- WBC 12.26 x10^3/μl N 73% L 22.3%
- CRP 16 (normal range 0 - 0.5)
- LDH 286 U/L
- CPK 202 U/L
- GOT 43 U/L
- TnI 1137.6 (<31ng/L).
- Swab for COVID-19 (24h)

Treatment
- Admitted to COVID-19 ward
- Treatment with hydroxychloroquine 200mg x 2 for seven days
- Azithromycin 500mg od for five days
- Darunavir-cobicistat 800mg/150mg od
- LMWH 6’000 X 2 (90 kg)
- Bisoprolol 2,5mg
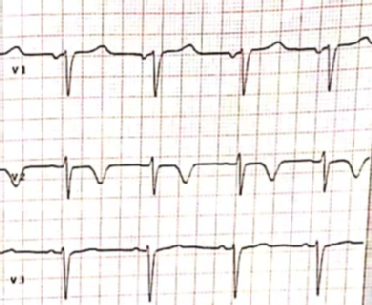
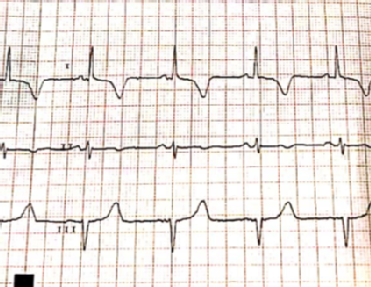
ECG
A new episode of chest pain after 12 hours.
SR, ST elevation in lateral leads with lateral negative T waves, Qtc 492msec.
Coronary angiography



No significant coronary artery stenosis.
Echocardiography
EF 50%, hypokinesis of lateral, anterior, and septal apical segments.
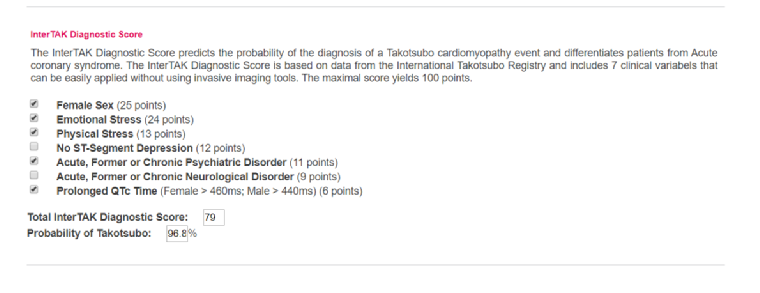
Differential diagnosis between Tako-Tsubo and myocarditis
- Husband died
- COVID-19 disease
The patient will undergo CMR the day after.
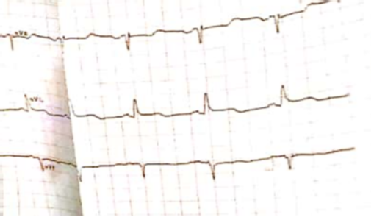
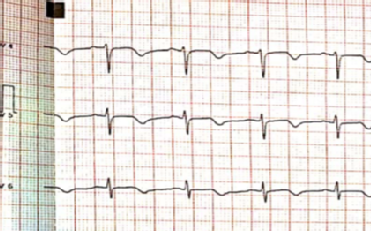
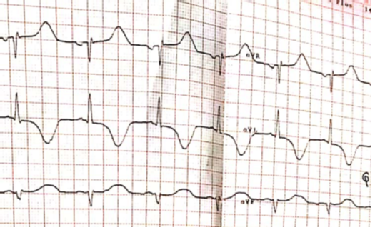
ECG after two days.
SR, Deep T waves inversion in lateral leads.
Clinical evolution
- Patient had not had new episodes of chest pain, hemodynamically stable
- Patient treated with ramipril, beta-blockers, aspirin and nitrates (high blood pressure) and COVID-19 treatment
- Improvement of pneumonia and oxygenation
- Improvement of lab exam
- Not performed biopsy (not available in our institution, not advisable moving the patient with COVID-19 positive during the outbreak)
- CMR will be performed soon (2-3 days)
Take-home messages
Extract from Barbara Casadei and Alida Caforio video
- Myocarditis is not a proven complication of COVID-19
- The diagnosis of myocarditis and of its cause is based on endomyocardial biopsy
- Abnormal troponin level does not equate to myocardial infarction in COVID-19
- No evidence-based treatment for COVID-19 complications - Need for randomised controlled trials
Brief report from JAMA Cardiology: Cardiac Involvement in a Patient With Coronavirus Disease 2019 (COVID-19) - 27 March 2020
Summary
- Tako-Tsubo syndrome (clinical presentation, risk factors, echocardiographic pattern)
- Can not exclude myocarditis (but very uncommon, until today on 1,000 patients still no clinically significant myocarditis found)
- Never underestimate chest pain in COVID-19
- Tako-Tsubo could affect COVID-19 patients (respiratory distress + Family clusters)
- Troponin can be positive for hypoxia but also for Minoca or ACS