

















Echocardiography plays an essential role in HCM, providing important information for prognosis, decision-making, sudden cardiac death stratification and assessment of response to medical or invasive therapies2. Here we will discuss the echocardiographic assessment of IVO in HCM.
Anatomy
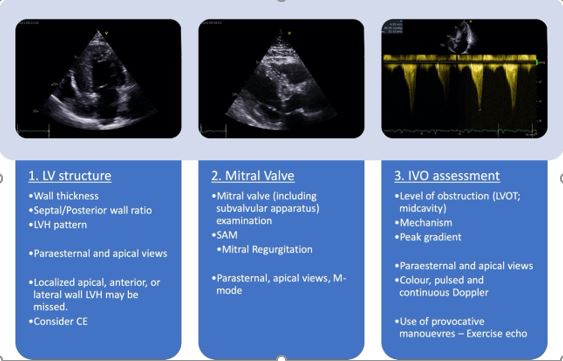
Patterns of hypertrophy, myocardial thickness and appearance
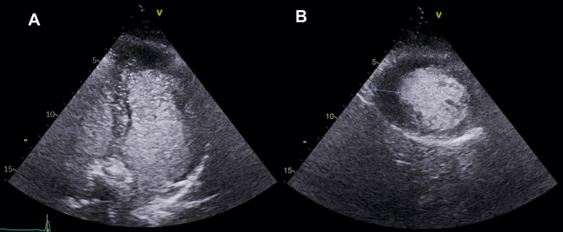
Left ventricular hypertrophy (LVH) is frequently limited to one myocardial segment and may present with a hyperechogenic appearance. To assess LVH it is advisable to use a standardised protocol that analyses all myocardial segments from base to apex. Measurements are made at end-diastole and are most accurate in short-axis views (although all available views should be used). Right ventricular (RV) wall thickness (WT) should also be measured. Contrast echocardiography (CE) is useful in localised forms of LVH, specifically in the apex and lateral wall. It also facilitates the identification of apical aneurysms, which are mainly seen in midventricular and apical obstruction3.
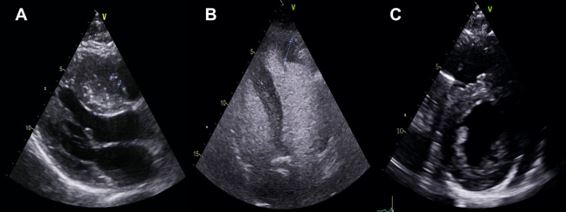
The echocardiographic evaluation should detail the distribution of LVH, being the more common patterns of distribution of LVH (Figure 1).
- Asymmetric septal hypertrophy (ASH): this is the most common pattern. The presence of septum ³15 mm and septum/posterior wall ratio 1.3/1 are characteristic of this type, although not pathognomonic. In children, more than two standard deviations above the mean adjusted for age, gender, and height. Technical errors in measurement, cutting the septum more obliquely on the parasternal long axis, may overestimate septal thickness.
- Concentric hypertrophy: symmetric LVH presents with similar measurements between septum, anterior and posterior free wall.
- Sigmoid septal: localised basal anteroseptal wall hypertrophy.
- Apical ventricular hypertrophy: less common in general. It is characterised by hypertrophy of the apical segments and a resultant “ace of spades” diastolic LV cavity in the apical 4-chamber axis. The diagnosis may be missed when the apical endocardium is not well visualised, and in these cases, CE unveils the diagnosis (Figure 2).
Mitral Valve Assessment
A comprehensive evaluation of the mitral valve apparatus is mandatory. A high percentage of patients have abnormal mitral leaflets and more than 25% show involvement of the subvalvular apparatus [chordae and papillary muscles (PM)]. Common abnormalities include leaflet elongation and excessive tissue, dysplasia and prolapse, chordal elongation, laxity and hypermobility; PM hypertrophy, bifidity, anterior or apical displacement, and direct insertion into the anterior the mitral valve leaflet4. Mitral systolic anterior motion (SAM) with an anterior mitral valve leaflet elongation (>16mm) increases the likelihood of left ventricular outflow tract obstruction (LVOTO).
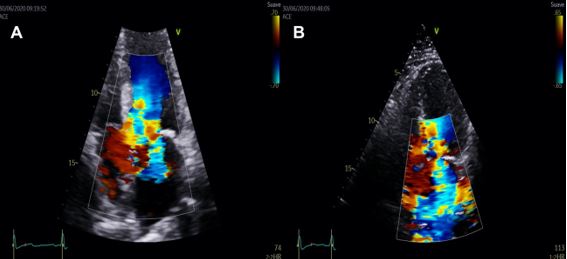
Mitral regurgitation (MR) may be influenced by secondary or primary mechanisms. Whereas MR due to annulus dilation or intrinsic valve disease may be central or anterior-directed, MR in context of SAM usually has a mid-to-late systolic onset, which interferes with the assessment of LVOTO5.
The mechanisms of MR in HCM include SAM with failure of leaflet coaptation, elongated mitral leaflets coapting in the leaflet body, anterior displacement of the mitral apparatus and PM. The anterior leaflet of the mitral valve behaves as an anterior prolapse and this arrangement in systole generates a typically mid-to-late onset eccentric lateral and posterior MR jet. Quantification of MR severity should be performed according to published recommendations and its dynamic components evaluated with provocative manoeuvres or EE3 (Figure 3).
Echocardiographic assessment of Intraventricular Obstruction
IVO is common in the LV (occurring at the left ventricular outflow tract (LVOT) or mid-cavity level) while it is infrequently seen in the RV.
Left Ventricular Outflow Tract Obstruction (LVOTO)
Certain anatomical variations of the left ventricular outflow tract and mitral valve area facilitate this phenomenon3,5:
- Narrowed diameter of the LVOT due to IVS hypertrophy
- Apically positioned papillary muscles that tether the mitral valve plane toward the ventricular septum
- Elongated anterior mitral valve leaflet
- Anterior displacement of the mitral apparatus
- Mitral systolic anterior motion (SAM) with leaflet-IVS contact in mid-systole.
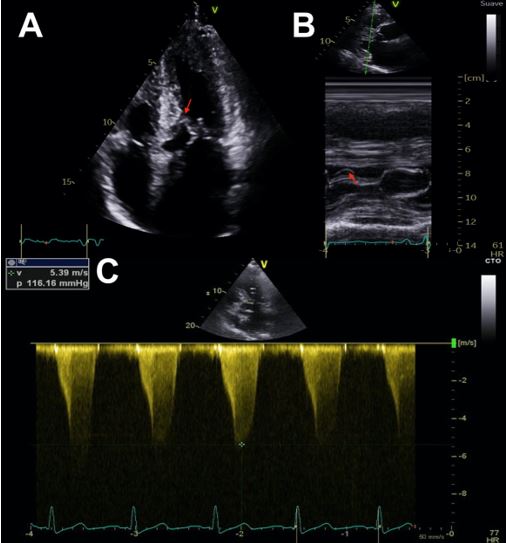
Colour Doppler is useful to initially locate the level at which the obstruction occurs, as aliasing will occur where there is flow acceleration. To measure LV outflow tract and intraventricular gradients, continuous Doppler is used to measuring the degree of obstruction and pulsed Doppler to locate the exact point where the obstruction is occurring, since depending on the different patterns of ventricular hypertrophy, the obstruction may occur at different levels. It is therefore advisable to use pulsed Doppler from the apex to the base and outflow tract so as not to miss possible intraventricular areas of increased gradients. The typical morphological appearance of the Doppler signal is a “dagger-shaped” and late peaking curve. This is because HCM creates a vicious circle in which obstruction generates more obstruction. At the beginning of systole, ejection begins normally but as systole progresses the outflow tract narrows due to increased pressure and the pressure increases further due to the narrowing of the outflow tract thus closing the circle. Thus, the continuous Doppler contour shows a progressive flow acceleration pattern (Figure 3).
Significant LVOTO is defined as a peak gradient ³ 30 mmHg (rest or provoked). About one-third of patients present LVOTO in resting conditions (obstructive HCM). In another third, LVOTO is only seen after provocative manoeuvres (provocable obstructive HCM) while the remaining third show no gradient at rest or after provocation (non-obstructive HCM). A resting or provocable peak gradient of 50mmHg or higher is considered the threshold for septal reduction procedure in symptomatic patients.
Midventricular obstructive HCM is a less common variant and is due to midventricular hypertrophy or anomalous PM insertion. Mid-systolic apposition of the septum and the lateral wall results in an “hourglass-shaped” LV chamber and a mid-cavity gradient. It is frequently associated with apical aneurysms and colour Doppler often shows flow in the sequestered area and a paradoxical apex-to-base diastolic gradient6.
Dynamic Nature of IVO: inducible obstructive HCM
IVO shows unpredictable and spontaneous variability and should be routinely assessed at rest and with bedside manoeuvres (Valsalva manoeuvre and standing). The use of nitrates should be reserved for patients who cannot perform or tolerate other manoeuvres and the use of dobutamine is not indicated since this infusion can induce LVOTO in normal subjects.
In patients who describe symptoms compatible with IVO in whom classic provocative manoeuvres fail to induce a gradient of 50 mmHg or higher, exercise echocardiography (EE) is recommended7. EE is feasible, safe and physiological, simulating real-life loading conditions and allowing integration of exercise tolerance symptoms, blood pressure and arrhythmias. It may also be considered in asymptomatic patients when diagnosis of IVO is relevant for lifestyle advice and treatment decision.
When the patient has reached peak exercise during EE, images are obtained early in the recovery period, when preloading decreases and IVO increases (within 60-90 seconds). We should a standardised protocol during EE, including assessment of LVOTO (prior to LV evaluation, as it is a short-lived phenomenon), MR and mitral anatomy (SAM), tricuspid regurgitation (to exclude exercise-induced pulmonary hypertension), LV systolic and diastolic function8.
Pitfalls assessing IVO
The diagnostic accuracy of echocardiography is not perfect and may result in false-negative and false-positive diagnosis. One important entity in the differential diagnosis of LVOTO, is a subaortic membrane. It should be suspected when there is a severe obstruction in the absence of SAM. Both in fixed and dynamic subaortic obstruction, the aortic valve may present a mid-systolic partial closure which is best documented with M-mode. Its presence, consequences on the aortic valve (mainly aortic regurgitation), and anatomical relationship with the mitral valve apparatus are better assessed with transoesophageal echocardiography (TOE). In addition, when quantifying LVOT gradient, care must be taken to avoid contamination with MR. Although not specific, MR typically shows an earlier onset, a complete parabolic contour (unlike the dagger-shaped contour of LVOTO gradient), and higher peak velocities. Finally, localized apical, anterior, or lateral wall LVH may be missed in patients with poor acoustic window (CE should be used whenever endocardial border imaging is suboptimal)3.
Conclusion
LVOTO (peak gradient ≥ 30 mmHg), either at rest or with provocation, is present in an elevated number of patients with HCM. Septal hypertrophy and anatomic alterations in the mitral apparatus are the main responsible for LVOTO. Echocardiography is essential in HCM assessment and provides information for prognosis and decision-making. It is recommended to use a standardised protocol with provocative manoeuvres to reveal LVOT in case it is not present at rest. Exercise echocardiography can be useful in whom classic provocative manoeuvres fail to induce a gradient of 50 mmHg or higher. Furthermore, it is feasible, safe and physiological, simulating real-life loading conditions