Paris, France – Aug. 30, 2011: Acute myocardial Infarction (AMI) is a major cause of death and disability. Worldwide, one in eight patients die of an ischemic heart disease. Its rapid and accurate diagnosis is critical for the initiation of effective evidence based medical management, including early revascularization, but is still an unmet clinical need. The gradual implementation of high-sensitive cardiac troponins (hs-cTnT) in clinical practice has helped clinicians to detect and treat patients with acute myocardial infarction earlier than with conventional assays. But, high-sensitive assays have also caused considerable confusion among clinicians as to the interpretation of, in particular, minor elevations. Now, many patients with cardiovascular disorders such as tachyarrhythmia, hypertensive urgency or heart failure are also “troponin positive” with the high-sensitive assays, in the absence of a coronary obstruction.
The findings emerged from the ongoing, international multicenter study APACE (Advantageous Predictors of Acute Coronary Syndrome Evaluation). Comprehensive characteristics of 887 patients, who had all presented to the emergency department with acute chest pain, were analysed. The investigators of this study focused on the clinically most challenging differential diagnosis in acute chest pain patients: AMI vs. cardiac, non-coronary diseases. They found out that by applying a simple algorithm, using presence of ST-elevation in the electrocardiogram, presentation values and changes of hs-cTnT in the first hour accurately distinguishes the two groups. Absolute changes of hs-cTnT were much more discriminatory than relative changes. Remarkably,
absolute changes of hs-cTnT as low as 0.005 mcg/l had the best discriminatory power in the differential diagnosis of AMI and cardiac, non-coronary diseases. 98.4% of all patients with AMI had either presentation values above 0.028 mcg/l or absolute changes of more than 0.005 mcg/l in the first hour.
Interestingly, considering changes of hs-cTnT after the first hour, does not seem to generate much further benefit.
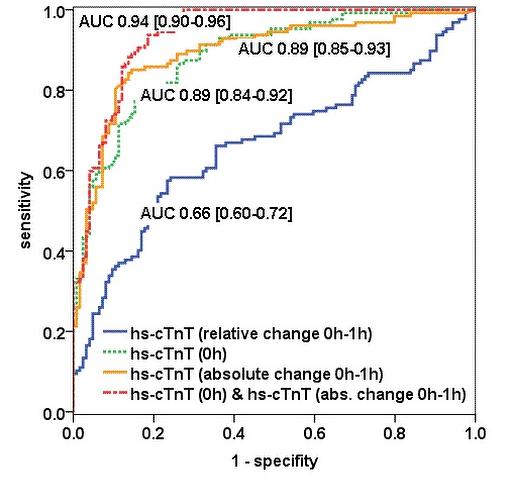
The high diagnostic accuracy of the combined use of hs-cTnT at presentation and at one hour, added up to an area under the curve of 0.94. In times of scarce resources, efficient allocation of invasive diagnostics will become more and more decisive in clinical practice. Patients presenting with acute chest pain are very different as to age and comorbidities and thus, their individual attitude regarding health and medical diagnostics in general. The level of pre-test probability necessary for further invasive diagnostic procedures – such as a coronary angiography – varies greatly between patients, but also physicians and was incorporated in a decision curve analysis.
The investigators showed that, again, the combined use of presentation values of hs-cTnT and its early change in the first hour was most helpful in order to properly allocate further invasive diagnostics to patients with acute chest pain and simultaneously leading to a substantial reduction in avoidable early coronary angiographies.
To sum it up, optimal troponin thresholds for hs-cTnT for therapeutic decision making – both at baseline and thereafter – remain a subject of debate. The application of the investigator’s algorithm may lead to earlier therapeutic decisions, shortening time of uncertainty for patients, more efficient use of financial resources and a substantial reduction in avoidable early coronary angiographies.
Figure 1: ROC Curve Analysis for the Differentiation between Acute Myocardial Infarction and Cardiac, but Not Coronary Diseases
Contributors:
Philip Haaf, MD1; Beatrice Drexler, MD1; Tobias Reichlin, MD1,2; Raphael Twerenbold, MD1; Miriam Reiter, MD1; Julia Meissner, MD1; Nora Schaub, MD1; Claudia Stelzig, MSc1; Michael Freese, RN1; Amely Heinzelmann, MD1; Christophe Meune, MD PhD1,3; Cathrin Balmelli, MD1; Heike Freidank, MD4; Katrin Winkler, MD5,6; Willibald Hochholzer, MD1,7; Kris Denhaerynck1 and Christian Mueller, MD1,2
1Department of Internal Medicine, University Hospital, Basel; 2Department of Cardiology, University Hospital, Basel; 3Paris Descartes University, Cardiology department, Cochin Hospital, APHP, Paris, France; 4Department of Laboratory Medicine, University Hospital, Basel, all in Switzerland; 5Servicio de Pneumologia, Hospital del Mar - IMIM, UPF, CIBERES, ISC III, Barcelona, Spain; 6Servicio de Urgencias, Hospital del Mar - IMIM, Barcelona, Spain; 7TIMI Study Group, Cardiovascular Division, Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA
Contact Details
Dr. Philip Haaf
Department of Cardiolgoy, University Hospital Basel
Petersgraben 4, CH-4031 Basel, Switzerland
Mobile: +41 76 20 484 57; Fax: +41 61 265 53 53 E-mail: haafp@uhbs.ch
Funding Sources
The study was supported by research grants from the Swiss National Science Foundation (PP00B-102853), the Swiss Heart Foundation, Abbott, Roche, Nanosphere, Siemens, and the Department of Internal Medicine, University Hospital Basel.