References
1. Stratton IM, Adler AI, Neil HA et al. (2000) Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. British Medical Journal 321(7258):405–412. 1. Stratton IM, Adler AI, Neil HA et al. (2000) Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. British Medical Journal 321(7258):405–412.
2. Diabetes Control and Complications Trial Research Group (1993) The effect of intensive diabetes treatment on the development and progression of long-term complications in insulin-dependent diabetes mellitus: the Diabetes Control and Complications Trial. New England Journal of Medicine 329:978–986
3. Morgan CL, Currie CJ, Peters JR. (2000) Relationship between diabetes and mortality: a population study using record linkage. Diabetes Care 23(8):1103–1107.
4. Riddle MC, Gerstein HC, Holman RR et al (2018) A1c targets should be personalised to maximise benefits while limiting risks. Diabetes Care 41:1121-1124
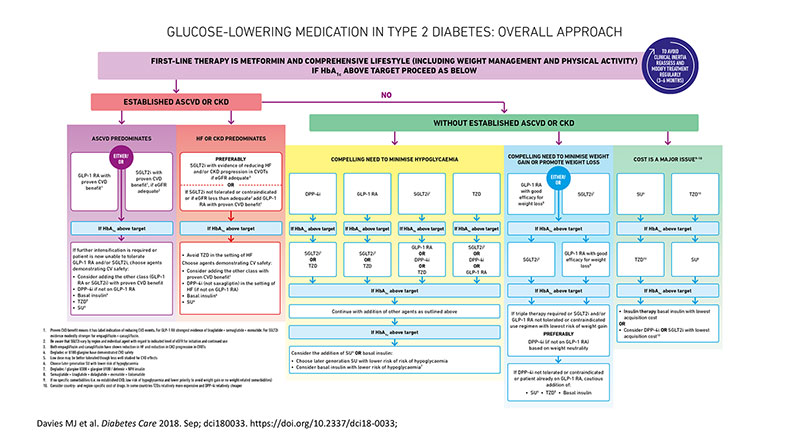
5. Davies MJ, D’Alessio DA, Fradkin J et al. (2018) Management of Hyperglycaemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) Diabetologia 61: 2461-2498
6. White NH, Sun W, Cleary PA, et al. (2008) Diabetes Control and Complications/Epidemiology of Diabetes Interventions and Complications Research Group. Prolonged effect of intensive therapy on the risk of retinopathy complications in patients with type 1 diabetes mellitus: 10 years after the Diabetes Control and Complications Trial. (EDIC)Arch Ophthalmol 126:1707–1715pmid:19064853
7. Hemmingsen B, Lund SS, Gluud C et al. (2011) Intensive glycaemic control for patients with type 2 diabetes: Systematic review with meta-analysis and trial sequential analysis of randomised clinical trials. British Medical Journal (Online).343 (7834) (pp 1136),
8. Reichard P, Nilsson B-Y, Rosenqvist U (1993) The effect of long-term intensified insulin treatment on the development of microvascular complications of diabetes mellitus. New England Journal of Medicine 329:304–309
9. Eastman RC, Javitt JC, Herman WH et al. (1997) Model of complications of NIDDM. II. Analysis of the health benefits and cost-effectiveness of treating NIDDM with the goal of normoglycemia. Diabetes Care 20: 735-44
10. Clarke PM, Gray AM, Briggs A et al. (2005) Cost-utility analyses of intensive blood glucose and tight blood pressure control in type 2 diabetes (UKPDS 72). Diabetologia 48: 868-77
11. Holman RR, Paul SK, Bethel MA et al. (2008) 10-year follow-up of intensive glucose control in type 2 diabetes. New England Journal of Medicine 359:1577–1589
12. UK Prospective Diabetes Study (UKPDS) Group (1998) Intensive blood glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complication in patients with type 2 diabetes (UKPDS 33). Lancet 352:837–853
13. UK Prospective Diabetes Study (UKPDS) Group (1998) Effect of intensive blood glucose control with metformin on complication in overweight patients with type 2 diabetes (UKPDS 34). Lancet 352:854–865
14. Turnbull FM, Abraira C, Anderson RJ, et al. (2009) Control Group. Intensive glucose control and macrovascular outcomes in type 2 diabetes. Diabetologia 52:2288–2298pmid:19655124
15. Ohkubo Y, Kishikawa H, Araki E et al (1995) Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with NIDDM: a randomized prospective 6-year study. Diabetes Research Clinical Practice 28:103–117
16. Mellbin LG, Rydén L, Riddle MC, et al.; ORIGIN Trial Investigators. Does hypoglycaemia increase the risk of cardiovascular events? A report from the ORIGIN trial. European Heart Journal 2013;34:3137–3144pmid:23999452
17. Standl E, Stevens SR, Armstrong PW, et al.; TECOS Study Group. Increased risk of severe hypoglycemic events before and after cardiovascular outcomes in TECOS suggests an at-risk type 2 diabetes frail patient phenotype. Diabetes Care 2018;41:596–603pmid:29311155
18. Gerstein HC, Miller ME, Byington RP, et al.; Action to Control Cardiovascular Risk in Diabetes Study Group. Effects of intensive glucose lowering in type 2 diabetes (ACCORD). New England Journal of Medicine 2008;358:2545–2559pmid:18539917
19. ADA (2018) 9. Cardiovascular disease and risk management: standards of medical care in diabetes- 2018 Diabetes Care 41:S86-S104
20. Marso SP, Daniels GH, Brown-Frandsen K, et al.; LEADER Steering Committee; LEADER Trial Investigators. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2016;375:311–322pmid:27295427
21. Marso SP, Bain SC, Consoli A, et al.; SUSTAIN-6 Investigators. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med 2016;375:1834–1844pmid:27633186
22. Zinman B, Wanner C, Lachin JM, et al.; EMPA-REG OUTCOME Investigators. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 2015;373:2117–2128pmid:26378978
23. Neal B, Perkovic V, Mahaffey KW, et al.; CANVAS Program Collaborative Group. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med 2017;377:644–657pmid:28605608
24. Wiviott SD, Raz I, Bonaca MP et al. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes (DECLARE-TIMI) N Engl J Med 2019; 380:347-357
25. Testa MA, Simonson DC. Health economic benefits and quality of life during improved glycemic control in patients with type 2 diabetes mellitus: a randomized, controlled, double-blind trial. JAMA 1998;280:1490–1496pmid:9809729
26. Kitabchi AE, Umpierrez GE, Miles JM et al. Hyperglycemic crises in adult patients with diabetes. Diabetes Care 2009;32:1335–1343pmid:19564476
27. International Diabetes Federation (IDF) Managing Older People With Type 2 Diabetes: Global Guideline 2013 available at: https://www.idf.org/component/attachments/attachments.html?id=985&task=download accessed January 2019
Bibliography:
Microvascular/Macrovascular complications:
Abbatecola AM, Rizzo MR, Barbieri M et al. (2006) Postprandial plasma glucose excursions and cognitive functioning in aged type 2 diabetics. Neurology 67: 235-40
Clarke PM, Gray AM, Briggs A. et al. (2004) A model to estimate the lifetime health outcomes of patients with type 2 diabetes: the United Kingdom Prospective Diabetes Study (UKPDS) Outcomes Model (UKPDS no. 68). Diabetologia 47: 1747-59
Clarke PM, Gray AM, Legood R et al. (2003) The impact of diabetes-related complications on healthcare costs: results from the United Kingdom Prospective Diabetes Study (UKPDS Study No. 65). Diabetic Medicine 20: 442-50
Morgan CL, Currie CJ, Peters JR. (2000) Relationship between diabetes and mortality: a population study using record linkage. Diabetes Care 23(8):1103–1107.
Reichard P, Nilsson B-Y, Rosenqvist U (1993) The effect of long-term intensified insulin treatment on the development of microvascular complications of diabetes mellitus. New England Journal of Medicine 329:304–309
Retinopathy:
Henricsson M, Nilsson A, Janzon L et al. (1997) The effect of glycaemic control and the introduction of insulin therapy on retinopathy in non-insulin-dependent diabetes mellitus. Diabetic Medicine 14: 123-31
Klein R, Klein BEK, Moss SE, Davis MD, DeMets DL (1988) Glycosylated hemoglobin predicts the incidence and progression of diabetic retinopathy. JAMA 260:2864–2871
Morisaki N, Watanabe S, Kobayashi J et al. (1994) Diabetic control and progression of retinopathy in elderly patients: five-year follow-up study. Journal of the American Geriatrics Society 42: 142-5
Nakagami T, Kawahara R, Hori S et al. (1997) Glycemic control and prevention of retinopathy in Japanese NIDDM patients. A 10-year follow-up study. Diabetes Care 20: 621-2
Cardiovascular diseases:
Adler AI, Neil HA, Manley SE et al. (1999) Hyperglycemia and hyperinsulinemia at diagnosis of diabetes and their association with subsequent cardiovascular disease in the United Kingdom prospective diabetes study (UKPDS 47). American Heart Journal 138: S353- S359
Advance Collaborative Group (2005) ADVANCE: Action in Diabetes and Vascular Disease: patient recruitment and characteristics of the study population at baseline. Diabet Med 22:882–888
Bastien A (2004) The ACCORD trial: a multidisciplinary approach to control cardiovascular risk in type 2 diabetes mellitus. Pract Diabetol 23:6–11
Bruno G, Merletti F, Boffetta P et al. (1999) Impact of glycaemic control, hypertension and insulin treatment on general and cause-specific mortality: an Italian population-based cohort of type II (non-insulin-dependent) diabetes mellitus. Diabetologia 42: 297-301
Eeg-Olofsson K, Cederholm J, Nilsson PM et al. (2010) New aspects of HbA1c as a risk factor for cardiovascular diseases in type 2 diabetes: an observational study from the Swedish National Diabetes Register (NDR). Journal of Internal Medicine 268: 471-82
Gerstein HC, Pogue J (2005) The relationship between dysglycaemia and cardiovascular and renal risk in diabetic and non-diabetic participants in the HOPE study: a prospective epidemiological analysis. Diabetologia 48: 1749-55
Hayward RA, Reaven PD, Wiitala WL, et al.; VADT Investigators. (2015) Follow-up of glycemic control and cardiovascular outcomes in type 2 diabetes. New England Journal of Medicine 372:2197–2206pmid:26039600
Kelly TN, Bazzano LA, Fonseca VA, et al. (2009) Systematic review: glucose control and cardiovascular disease in type 2 diabetes. Ann Intern Med 151:394–403pmid:19620144
Molyneaux LM, Constantino MI, McGill M et al. (1998) Better glycaemic control and risk reduction of diabetic complications in Type 2 diabetes: comparison with the DCCT. Diabetes Research & Clinical Practice 42: 77-83
Nakamura T, Matsuda, T, Kawagoe, Y et al. (2004) Effect of pioglitazone on carotid intimamedia thickness and arterial stiffness in type 2 diabetic nephropathy patients. Metabolism: clinical and experimental 53: 1382-1386 (Abstract).
Nathan DM, Turgeon H, Regan S (2007) Relationship between glycated haemoglobin levels and mean glucose levels over time. Diabetologia 50: 2239-44
General diabetes:
American Diabetes Association (2006) Standards of medical care in diabetes—2006. Diabetes Care 29(Suppl 1):S4–42
Chapell R, Gould AL, Alexander CM (2009) Baseline differences in A1C explain apparent differences in efficacy of sitagliptin, rosiglitazone and pioglitazone. Diabetes Obesity and Metabolism 11: 1009-16
Clarke PM, Gray AM, Holman RR (2002) Estimating utility values for health states of type 2 diabetic patients using the EQ-5D (UKPDS 62). Medical Decision Making 22: 340-9
International Diabetes Federation (2011) Definition and diagnosis of diabetes mellitus and immediate hyperglycemia: report of a WHO/IDF consultation.
International Diabetes Federation. Definition and diagnosis of diabetes mellitus and immediate hyperglycemia: report of a WHO/IDF consultation. Geneva: World Health Organisation, 2006.
Iribarren C, Karter AJ, Go AS et al. (2001) Glycemic control and heart failure among adult patients with diabetes. Circulation 103: 2668-73
Little RR, Rohlfing CL, Wiedmeyer H-M, Myers GL, Sacks DB, Goldstein DE (2001) The National Glycohemoglobin Standardization Program (NGSP): a five year progress report. Clin Chem 47:1985–1992
Moreland EC, Volkening LK, Lawlor MT et al. (2006) Use of a blood glucose monitoring manual to enhance monitoring adherence in adults with diabetes: a randomized controlled trial. Archives of Internal Medicine 166: 689-95
Oglesby AK, Secnik K, Barron J, Al-Zakwani I, Lage MJ. The association between diabetes related medical costs and glycemic control: A retrospective analysis. Cost Effectiveness & Resource Allocation 2006;4:1.
Qaseem A, Wilt TJ, Kansagara D, et al. (2018) Clinical Guidelines Committee of the American College of Physicians. Hemoglobin A1c targets for glycemic control with pharmacologic therapy for nonpregnant adults with type 2 diabetes mellitus: a guidance statement update from the American College of Physicians. Ann Intern Med. 6 March 2018 [Epub ahead of print]. DOI: 10.7326/M17-0939pmid:29507945
Hypoglycaemia:
Lim S, Kang SM, Shin H et al. (2011) Improved glycemic control without hypoglycemia in elderly diabetic patients using the ubiquitous healthcare service, a new medical information system. Diabetes Care 34: 308-13
Self-monitoring:
Allen BT, DeLong ER, Feussner JR (1990) Impact of glucose self-monitoring on non-insulintreated patients with type II diabetes mellitus. Randomized controlled trial comparing blood and urine testing. Diabetes Care 13: 1044-50