
The recent advent of new cardiovascular imaging techniques has enlarged the diagnostic capabilities for any cardiologist. Nevertheless, due to the huge number of methods and techniques, it is very difficult for a physician to be permanently updated. During this ESC Congress and WCC 2006, many studies regarding cardiovascular imaging were presented. Summarising, the most striking advances can be divided into three categories: echo-Doppler, cardiac-CT and cardiac-MRI.
Echo-Doppler
During this congress, new techniques and applications of 3D echo have been shown. We have seen the role of 3D echo in the assessment of left ventricular volume, morphology and function. Furthermore, 3D echo allows a global, fast and accurate assessment of the left ventricle based on the semi-automated endocardial border tracking technique (1) (figures 1 and 2). These capabilities can be used to evaluate mechanical cardiac asynchrony and the response of patients to cardiac resynchronization therapy. One of the most recent advances in the field of 3D echo is the development of the parametric imaging. Using this new feature, it is possible to analyze left ventricular movement and synchrony only looking a color-coded image as the one represented in figure 2 (2).
Another new advance presented during this congress was the speckle-tracking analysis (3). This method allows - in a very friendly manner - to assess changes in length, velocity, acceleration, strain and strain-rate analysing the cardiac walls. Thus, this method can obtain direct measurements of strain and strain rate. Until now we could only obtain these measurements by deriving their values from tissue Doppler data sets.
And there were also several studies concerning the role of echo-Doppler to assess the effect of cell-therapy, its usefulness to assess the morphology and function of the left atrium and new advances regarding old subjects such as valvular heart disease, the usefulness of echo contrast for left ventricular opacificación and perfusion and stress echo (4).
Cardiac-CT
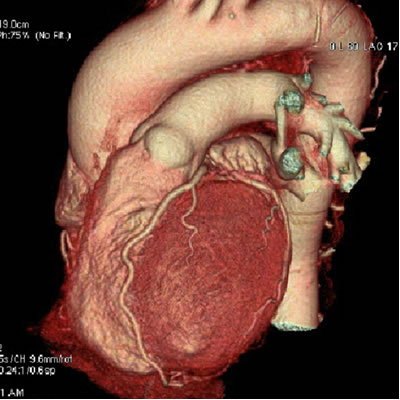
One of the most emphasised subjects regarding cardiovascular imaging in this congress has been cardiac-CT. This new image modality is emerging as a diagnostic tool for global assessment not only of the heart but the complete cardiovascular system. With the development of the 64-slice cardiac-CT, is possible to evaluate cardiac morphology and function as well as coronary and by-pass graft anatomy (5).
During this congress, several studies evaluating the diagnostic accuracy ofcardiac-CT using coronary angiography stress imaging tests as reference method were covered. Doubts have been raised concerning the prognostic usefulness of a coronary calcium score. But the majority of the studies have shown the role of 64-slice cardiac-CT over 16-slice cardiac-CT (figure 3), its usefulness as a screening tool for coronary artery disease in different scenarios, its usefulness on patients with coronary stents, its capability to analyse atherosclerotic plaques (burden, distribution, characteristics,…) and its new applications, to evaluate aortic valvular stenosis for instance (6).
Cardiac-MRI
And finally, a large number of abstracts analysing the diagnostic capabilities of cardiac-MRI were presented. In various abstracts presentations and conferences, the role for tissue characterisation of cardiac-MRI was presented not only in patients with ischemic heart disease, but in patients with different cardiomyopathies (7). The usefulness of cardiac-MRI to evaluate a new and promising therapeutic method, the cell therapy, was also established as well as its accuracy for the evaluation of valvular heart disease (8). Furthermore, cardiac-MRI has been established again as a “one stop shop” to evaluate cardiovascular disease.
Figure 1: Left ventricular “cast” obtained from real-time 3D echo datasets and time-volume curve representing left ventricular global volume change over the cardiac cycle.
Figure 2: Left ventricular “cast” obtained from real-time 3D echo datasets and time-volume curves representing left ventricular regional volume changes over the cardiac cycle.
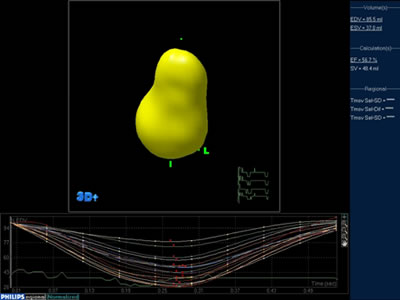
Figure 3: Parametric images representing left ventricular excursion and asynchrony obtained from real-time 3D echo datasets. This figures are automatically displayed by the new 3D echo software.
Figure 4: Coronary angiography obtained by using 64-slice cardiac-CT.
The content of this article reflects the personal opinion of the author/s and is not necessarily the official position of the European Society of Cardiology.