















Abbreviations
CA: catheter ablation
AF: atrial fibrillation
PVI: pulmonary vein isolation
RF: radiofrequency
CB: cryoballoon
HF: heart failure
LVEF: left ventricular ejection fraction
NOAC: vitamin K oral anticoagulants
Introduction
Atrial fibrillation (AF) is the most common arrhythmia with a rapidly rising global prevalence due mainly to the aging world population. Patients with AF often experience significant impairment in their quality of life and more importantly, they have an increased risk for adverse cardiovascular outcomes (stroke, heart failure, cardiac death) [1]. Rhythm control (i.e., restoration of sinus rhythm and prevention of new AF episodes) is an integral part of the therapeutic approach as proposed in the recent ESC Guidelines, along with anticoagulation, rate control of the tachyarrhythmia, and treatment of the cardiovascular risk factors and the AF associated co-morbidities [2]. Antiarrhythmic drugs have been widely used for rhythm control in AF, albeit with limited success. On the other hand, CA has emerged as the first-choice treatment strategy with the rapid development of new techniques over the recent decades.
Atrial fibrillation ablation: methods
AF ablation approaches are based upon our current understanding of the underlying mechanisms of this complex arrhythmia. The importance of ectopic activations originating mainly in the pulmonary veins is widely recognised as the mechanism responsible for the initiation of AF. Accordingly, the electric isolation of the pulmonary veins, introduced by Haissaguerre and colleagues in the late '90s, remains the predominant ablation strategy for both paroxysmal and persistent AF [3]. On the other hand, the mechanisms sustaining AF are only partially understood. As a consequence, ablation strategies aiming to eliminate these mechanisms vary substantially and are in general less successful in comparison to pulmonary vein isolation (PVI). These later approaches include the ablation of wide areas of atrial tissue (atrial roof, posterior wall, and mitral isthmus, left atrial appendage) to minimise the substrate required to sustain AF or the ablation of specific focal activity areas with centrifugal expansion (rotors) [4].
Two ablation techniques are currently used when performing PVI: point-by-point radiofrequency (RF) ablation of the atrial tissue surrounding the pulmonary veins using a single-point catheter and a three-dimensional (3D) mapping system (Figure 1) or ``single-shot`` ablation with the use of a cryoballoon (CB) (Figure 2). Each method has its advantages and disadvantages, but neither is superior to the other concerning safety or efficacy in the treatment of paroxysmal AF as shown in the FIRE AND ICE trial [5]. A big advantage of the RF-based approach is that it can be used to ablate atrial tissue beyond PVI, a common practice for the treatment of long persistent AF or recurrent AF after a first PVI attempt. However, the role of atrial ablation in addition to PVI versus PVI alone for the treatment of persistent AF has not been fully clarified [6]. Thus, PVI (with RF or CB) remains the first-line treatment strategy for both paroxysmal and persistent AF (Class I indication) with additional ablation lines carrying a Class IIb indication in the recent 2020 ESC AF guidelines [2].
Figure 1. Electroanatomical three-dimensional mapping of circumferential point-by-point pulmonary vein isolation. Dots represent the ablation points.
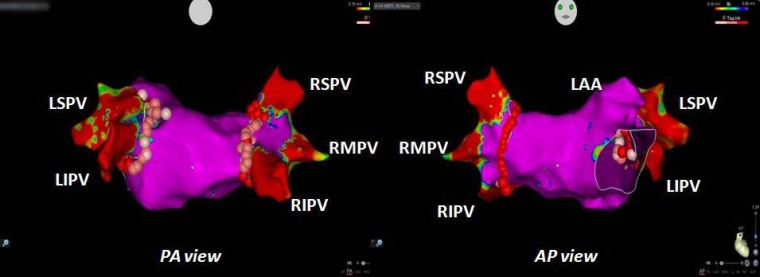
AP: antero-posterior; LAA: left atrial appendage; LSPV: left superior pulmonary vein; LIPV: left inferior pulmonary vein; PA: posterior-anterior; RSPV: right superior pulmonary vein; RIPV: right inferior pulmonary vein; RMPV: right middle pulmonary vein
Figure 2. Cryoablation of the left superior pulmonary vein. The Lasso catheter has been advanced inside the vein for support. The cryoballoon occludes the pulmonary vein.
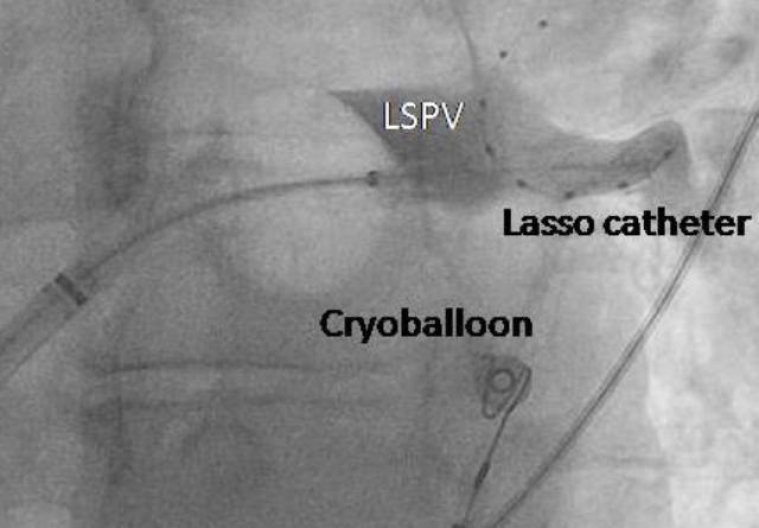
LSPV: left superior pulmonary vein
Atrial fibrillation ablation: efficacy, outcome, and safety
Elimination of the late recurrences and significant decrease of the AF burden are the two standard measures of success after CA. The 2017 expert consensus statement on catheter and surgical ablation of AF defined late recurrences of AF as the development of any type of atrial arrhythmia lasting more than 30 seconds (AF, atrial flutter, or atrial tachycardia) between 3-12 months post-ablation [7]. AF burden is measured as the proportion of time spent in AF during a prespecified monitoring period. It should be noted that early recurrences of AF that happen within the first 3 months of follow-up are of limited clinical importance since only half of those patients will finally develop later episodes of AF. Based on the above success measures several clinical trials have shown that a first AF ablation procedure can eliminate late recurrences in approximately 60-70% of patients with paroxysmal AF and decrease the AF burden by 70-90% in a follow-up ranging from 12 to 60 months. Success rates are typically lower in patients with persistent AF reaching 50% after a single procedure [8].
Several studies have shown that CA is more effective than antiarrhythmic medications in improving quality of life indices in symptomatic patients. The existing evidence is based on randomised trials with a follow-up period ranging from 6 months to 5 years [9]. This beneficial effect has not been necessarily associated with the elimination of AF recurrences but rather with a significant reduction in arrhythmia burden [10].
In terms of clinical outcomes, recent evidence suggests a potential prognostic benefit of CA. Studies from the early 2000s, like the AFFIRM trial, failed to prove the superiority of rhythm versus rate control. This has been attributed to the adverse effects of antiarrhythmics which might have confounded a potential positive effect of the rhythm control strategy [11].
Even the recent large prospective multicentre CABANA trial which compared CA versus medical treatment in patients with paroxysmal and persistent AF and which showed clear superiority of CA for the prevention of recurrent atrial arrhythmias and the reduction of AF burden, failed to demonstrate a superiority of CA in the prevention of death, disabling stroke, serious bleeding, or cardiac arrest. However, a major caveat of this study was the cross-over of approximately 30% of the participants from the drug treatment group to the ablation arm [12].
On the other hand, in the EAST-AFNET 4 study which randomised AF patients within one year from initial diagnosis to either rhythm (with CA or with antiarrhythmic medications) or rate control, a more significant reduction in the primary composite endpoint of cardiovascular death, stroke or hospitalisation from worsening heart failure was observed in the rhythm control group after a median follow-up of 5 years. This was the first study that showed an improvement in the clinical outcome of AF patients (even asymptomatic ones) with an early rhythm control strategy. An association between clinical outcome and reduction in AF burden could not be shown since information about a recurrence of atrial arrhythmias was available only in the rhythm control group [13].
AF ablation is a relatively safe procedure with a complication rate varying between 2-3.5%. Nevertheless, life-threatening complications, although rare, can occur. In-hospital mortality following ablation varies between 0.6 and 4 per 1,000 patients [14]. Cardiac tamponade is the most frequent serious complication leading to death, while local vascular complications are the most common adverse effect related to the procedure. Other complications include pulmonary vein stenosis, catheter entrapment, periprocedural embolic events, phrenic nerve injury, atrioesophageal fistula, vagal nerve injury, acute coronary artery injury, and pericarditis. Advanced age, obesity, and cardiovascular comorbidities have all been associated with an adverse outcome after CA.
Ablation of atrial fibrillation in patients with heart failure
Catheter ablation can be particularly challenging in patients with AF and heart failure (HF) due to the expected increased risk for intra-procedural complications and arrhythmia recurrence. However, patients with HF seem to benefit the most from this procedure. The development of AF is associated with a significant deterioration in the haemodynamic indices and an increase in morbidity and mortality of patients with HF. On the other hand, HF seems to promote the development of AF. Several smaller observational studies and randomised control trials have clearly shown that CA is associated with a significant decrease in arrhythmia burden, an improvement of left ventricular ejection fraction (LVEF), and also an improvement in the quality of life of patients with HF, even in those with preserved left ventricular systolic function.
The seminal CASTLE-AF study was the first trial to demonstrate a significant reduction in mortality with CA in comparison to medical care in patients with AF. This study randomised patients with LVEF <35%, and symptomatic paroxysmal or persistent AF to CA or medical care. A significant reduction in the composite endpoint of death or hospitalisation for worsening HF (28.5% vs 44.6%) after a mean follow-up of 38.7 months was observed in the ablation group and was attributed mainly to a significant reduction in cardiovascular deaths [15]. A subgroup analysis of the CABANA trial further confirmed the beneficial effect of CA regarding morbidity and mortality of patients with reduced EF [16]. Based on these findings the ESC has given a Class IIa indication to CA for AF patients with HF and reduced LVEF in the 2020 AF guidelines [2]. More importantly, a recent subanalysis of the EAST – AFNET 4 trial showed that rhythm control therapy within a year from the first diagnosis of AF reduces cardiovascular events in patients with signs or symptoms of heart failure even in patients with preserved ejection fraction [17].
Atrial fibrillation ablation: who is the best candidate?
In seeking the AF patient who will gain the most benefit from a CA treatment strategy several factors have to be taken into account. The low probability of arrhythmia recurrence, the improvement in the quality of life, and the decrease in the long-term morbidity and mortality should be combined with the lowest possible risk of intra- and post-procedural complications. Advanced age, long AF duration (long persistent AF, CA>1 year after the initial diagnosis), left ventricular systolic dysfunction (EF<25%), increased left atrial size (diameter >5 cm), and the presence of comorbidities (obesity, hypertension, metabolic syndrome, obstructive sleep apnoea) are the main factors predicting a high recurrence rate of atrial arrhythmias post-ablation. However, none of the above factors is an absolute contraindication to CA. Only in the presence of left atrial thrombus is the procedure contraindicated.
Of note, recent data have shown that CA can be safely performed in selected low-risk AF patients under uninterrupted anticoagulation with the new non-vitamin K oral anticoagulants (NOACS) without the need for pre-or peri-procedural transoesophageal echocardiography to exclude the presence of atrial thrombus [18]. Regarding CA in the elderly, although AF is more prevalent in the elderly population, older patients (>75 years) have been generally underrepresented in the large clinical trials of CA. Accumulated evidence from several small studies has shown that both safety and efficacy of CA are marginally inferior in this age group in comparison with younger AF patients, while vascular complications and the need for antiarrhythmic drugs after CA may be slightly higher [19]. Regarding the clinical benefit of CA, the data are rather scarce and controversial. An improvement in symptoms as well in morbidity and mortality has been reported in some small non-randomised studies [20].
Based on the above, the ideal candidate for CA would be the relatively young patient with several symptomatic episodes of paroxysmal AF of recent onset (<1 year) and without comorbidities or signs of structural remodelling of the heart (normal LVEF, no or minimal atrial enlargement). Although the majority of AF patients undergoing ablation in everyday clinical practice do not fulfil all these criteria, most experience a beneficial effect. New technologies are underway intending to improve the effectiveness, efficiency, and safety of CA and to increase the success rate even for AF patients who are currently considered poor candidates for this treatment strategy.
Conclusions and take-home messages
Catheter ablation is more effective than antiarrhythmic drugs for rhythm control in patients with AF and can be considered as a first-line treatment for symptomatic patients with paroxysmal or persistent AF.
Pulmonary vein isolation is the preferred ablation technique for patients with either paroxysmal or persistent AF. More extensive left atrial ablation for long persistent AF or more commonly for recurrence after a first PVI procedure is currently in practice in many centres although the evidence supporting this strategy is rather weak.
Several studies have shown a significant improvement in the quality of life of patients with AF after CA. Since in a recent randomised trial, early rhythm control strategy (with CA or antiarrhythmic medications) reduced morbidity and mortality in patients with AF, further studies are needed to delineate the effect of CA on hard clinical endpoints such as cardiovascular morbidity and mortality.
Patients with HF and AF seem to benefit even more from CA. Several studies have shown not only an improvement in haemodynamics and left ventricular function but also a significant reduction in morbidity and mortality with CA.
Catheter ablation for the treatment of AF is relatively safe and effective also in patients older than 75 years. The long-term outcome may be favourable but the available evidence is rather weak.
Recurrence of atrial arrhythmias 3 months after the procedure (late recurrence) occurs more often in patients with long persistent AF or treated more than 1 year after the initial diagnosis. Advanced age, comorbidities, and the presence of structural remodelling of the heart are additional strong predictors of AF recurrence post-ablation.