

















Introduction
Cardiac electrophysiology was often described as a Cinderella speciality, with the work being done in darkened rooms, often discreet to the main department. Indeed, cardiac electrophysiologists looked more like nerds coding software than clinical physicians. Their activity was to recognise the mechanisms of cardiac arrhythmias using endocardial electrograms; the importance of a difference of a few thousandths of a second seemed ridiculous to those outside the field. Their interventional cardiologist colleagues readily mistook them for quirky explorers trying to decipher a text in an unknown language. In the beginning the electrophysiologist had very few treatments, performing diagnostic studies only, or seeing the effects of intravenous pharmaceuticals.
This remained true until the serendipitous discovery of ablation, and the subsequent refinement through radiofrequency ablation. Although capacity kept up with demand when the arrhythmias that could be treated were relatively limited, the advent of successful ablation strategies for atrial fibrillation (AF) and ventricular tachycardia (VT) led to an exponential increase in demand.
With the prevalence of atrial fibrillation far exceeding that of other arrhythmias, treating patients with AF now forms the majority of the working time of cardiac electrophysiologists. It was soon apparent that given the demand for treatment, AF ablation would have to become a simpler, safer, and more efficient procedure. This was a task taken up with relish by the community, just as it had been earlier for reentrant tachycardias, which initially took several hours, if not all day, to complete. While most patients with AF are stable, patients with VT, in contrast, are often very unwell, and long duration procedures can be counterproductive.
This need opened up a very important market in which engineers, manufacturers and doctors have rushed to improve, with clear improvements made over the last decade.
Where were we in 2010?
In 2010, I was a fellow at Guy’s St Thomas hospital and Dr Matt Wright was my mentor. At that time, the diagnosis and treatment of typical flutters (clockwise or anticlockwise) and nodal-related supraventricular tachycardia (AVRT, AVNRT) had been mastered. But AF and VT ablation, although well-established in the electrophysiology laboratory (EP lab), were sometimes unsuccessful and often complicated procedures. Some diagnoses of atypical flutters were not fully understood in all their complexity.
In addition, the holy grail was to complete permanent, transmural lesions, especially in the left atrium without the risk of reconnection, yet at the same time being controlled without extracardiac ablation. As there was no reliable way to measure the contact of the catheter with the underlying myocardium, the only feedback to the operator was the tactile sensation - learned over the course of thousands of procedures - of the catheter motion during the application using either fluoroscopy or 3D electroanatomic mapping (which was still in its relative infancy). Impedance changes could be measured, temperature changes likewise, but at the time these recordings were relatively crude.
Furthermore, each centre had its own recipe for the application of radiofrequency (RF) by varying the power, duration and target temperature. There was no evidence to help standardise the application of RF energy. Moreover, some areas of the heart (i.e., left ventricular summit, mitral isthmus, papillary muscle) had poor accessibility. That led to frustration amongst the electrophysiologists since the guilty conduction was recognised but was unable to be treated.
Speed and ease of diagnosis of complex arrhythmias
The principle of diagnosis in electrophysiology is to find the critical culprit anatomical site of the patient's clinical arrhythmia. It is the process of combining anatomy with the electrocardiogram.
Initially, the anatomical positioning of catheters was carried out under fluoroscopic guidance, with the operator having to mould the shape of the catheters themselves to try and get to the relevant place. In the 1990s, steerable and multi-electrode catheters enabled rapid diagnosis of supraventricular tachycardia, notably by analysing real-time activation in the coronary sinus or in the right atrium (Figure 1).
Figure 1. Rise of high-definition mapping for the diagnosis of complex arrhythmias during the last decade.
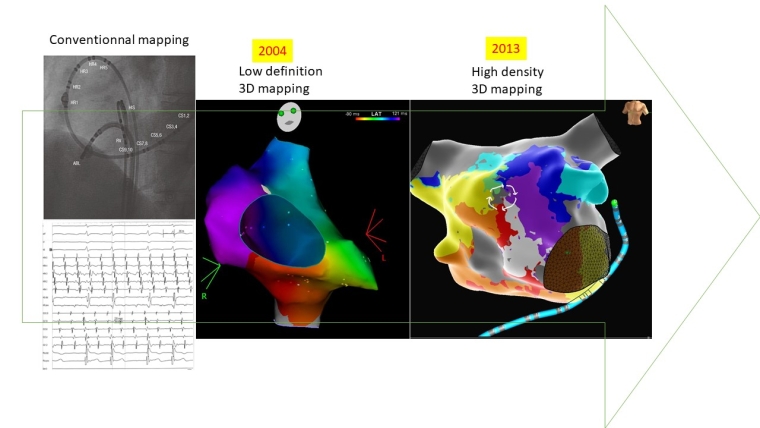
However, the increasing complexity of AF and VT ablation procedures required the need for three-dimensional visualisation. Thus, in the 2000s, electroanatomic 3D mapping systems (EAM) brought more precision and less need for fluoroscopy. Today, several systems exist in the market, each with their own strengths and weaknesses. These systems are able to create a three-dimensional space of the cardiac chamber of interest and display in real-time clinical arrhythmia activation maps (Figure 1) or voltage maps that allow an estimation of the substrate of the arrhythmia. While measuring the 3D anatomical space and assigning an electrogram to each area is relatively simple, there has been a lot of work to try and see beyond just the simple electrogram. The holy grail of AF is to try and find the source of what perpetuates the arrhythmia. Whether a single source is stable, or even exists is up for debate; so far, no system for analysis beyond the timing and amplitude of a stable single has stood the test of time.
The next development that would stand the test of time was multi-electrode mapping using the 3D electroanatomic mapping systems. In 2014, Patel et al demonstrated that the use of a 5-spline catheter (Pentaray; Biosense Webster) that performed simultaneous annotation of 20 sites at a time allowed for much faster mapping and subsequent diagnosis [1].
High-density (HD) mapping was quickly put to use for the ablation of ventricular tachycardia, in particular to get a precise idea of the ventricular substrate (in terms of low- voltage areas, often with slow conduction in sinus rhythm on non-mappable or noninducible VT) [2]. HD mapping remains a powerful tool for understanding micro- and macro- reentrant tachycardia and accurately detecting the critical site - the key to successful ablation - when standard catheters have failed. These benefits are largely due to the arrangement of small, closely spaced electrodes on these new catheters, in addition to the ability to measure the activation vector [3]. Coupled with intelligent algorithms, HD mapping enables rapid acquisition of a very precise arrhythmia map, although no randomised studies on the possible benefits of these new catheters have been published. However, in our experience, this is a tool to save procedural time with optimal precision. It was on this occasion that the double-loop and figure-8 phenomena in reentrant arrhythmia were highlighted (Figure 1).
Better RF delivery
Contact force catheter...
In the early 1990s, Dr David Haines demonstrated that the contact between the catheter and the tissue is a major determinant of the size of the lesion and the effectiveness of the ablation. Increasing contact improves the efficiency of RF ablation procedures. Too much contact however, increased the risk of tissue distortion and further complications: tamponade, damage to adjacent structures (atrioesophageal fistula, phrenic nerve palsy), pop, char and thrombus.
As a result, the ability to measure tissue contact during radiofrequency was crucial for efficiency as well as for safety. It was clear that with the massive demand for procedures, the learning curve had to be made easier than spending thousands of hours mastering the techniques.
In 2012, the first catheters sensitive to the contact force based on local electromagnetic parameters (SmartTouch; Biosense Webster) appeared, quickly followed by its competitor based on fibre optic technology (Tacticath; St. Jude Medical).
Clinical studies (TOCCASTAR [4], TOUCHAF [5]) followed suit, demonstrating better procedural parameters (RF time, procedure time, fluoroscopy time) with appropriate contact. However, these studies failed to show any long-term benefit. Apparent discrepancies between better techniques failing to demonstrate benefits in studies has long been seen in operative fields. While no one would now doubt the use of contact force sensing, at the time there was scepticism, fuelled in some part by the negative studies as well as the additional cost.
What is clear is that when novel technologies are trialled with key opinion leaders, with decades of experience, the benefits they experience are more marginal than for the majority of operators who do not have such experience. Importantly, these studies provided an understanding of the quality criteria for an efficient RF lesion (spatiotemporal dynamics: catheter stability, cardiac and respiratory motion, catheter drift).
...leading to smarter RF algorithms- “a recipe at last” ...
Quite quickly, around 2016-2017, more complex markers integrating criteria beyond simple contact appeared. These include a combination of catheter orientation with tissue and force directionality, RF power and time, impedance fall, lesion continuity and contiguity (interlesion distance), homogeneity of force, and presumed tissue thickness. Although the majority of electrophysiologists use these criteria (Ablation Index or Lesion Index) on a daily basis, randomised trials have failed to show superiority, probably for the reasons outlined above. Further studies are under way that incorporate the aforementioned metrics, apart from CF alone, on optimising ablation outcomes.
...leading to high power short duration (HPSD) ablation.
One of the consequences of these new algorithms was HPSD ablation. Since the quality of the lesion included several parameters including duration and power, one could easily imagine that more powerful RF with a shorter duration could be at least as effective. Around 2017-2018, high-power, short-duration (HPSD) ablation for the treatment of AF emerged as an alternative to conventional ablation generator settings, characterised by lower power and a longer duration (see Figure 2).
Figure 2. Evolution of the catheter technologies during the last decade.
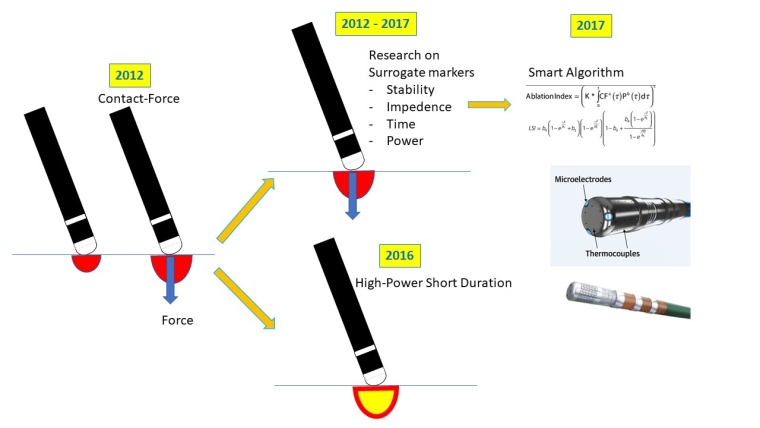
Although the reported potential advantages of HPSD ablation include less tissue oedema and collateral tissue damage, a reduction in procedural time and superior ablation lesion formation [6], clinical studies of HPSD ablation validating these observations are limited. One of the main challenges for HPSD ablation has been the inability to adequately assess temperature and lesion formation in real time. Novel catheter designs may improve the accuracy of intra-ablation temperature recording and correspondingly may improve the safety profile of HPSD ablation. Clinical studies of HPSD ablation are on-going [7] and interpretation of the data from these and other studies will be required to ascertain the clinical value of HPSD ablation.
Improved access to the target myocardium
From irrigated RF...
Initially, the only target areas for ablation were the endocardial sides of the heart chambers. Since the 1990s, the epicardial puncture technique has allowed a fresh look into the epicardial side of the heart.
Advances in mapping made it possible to understand that some arrhythmogenic substrates were truly intramural. Since 2010-2011, the aim of many published articles publications was to seek the necessary tools in order to obtain deeper lesions and reach the mid-myocardial portions of the heart walls.
... to “super” RF...
After the irrigated-tip ablation catheters that provided larger lesions, newer techniques have been developed for deeper RF lesions. External irrigation with normal saline may decrease lesion size by dispersing the radiofrequency current density. Alternative irrigation fluids such as half-normal saline with impedance modulation (additional surface dispersive electrode patches on patients) are able to create larger lesions. Even though safety and efficacy have been reported prospectively (Figure 3) when targeting deep myocardial substrate with half-normal saline, ablation safety concerns have appeared when combined with lowered impedance, and high-power settings [8].
Figure 3. Evolution of ablation technique for deep targets during the last decade.
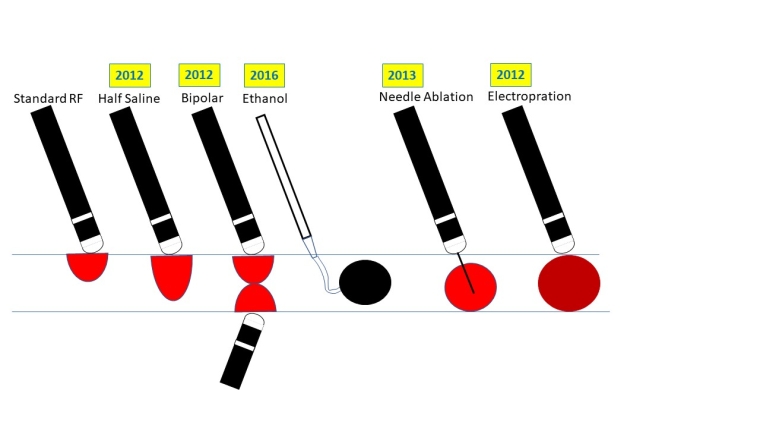
Standard unipolar RF ablation uses a single catheter from which current flows to large return patches at the body surface. Two catheters for either simultaneous unipolar ablation or bipolar ablation can be used to achieve transmural lesions. Both techniques have been reported in a small case series to successfully terminate VT in patients who had unsuccessful sequential unipolar ablation in septal and free wall VTs [9].
Finally, another investigational tool developed for deeper lesion formation uses a catheter with an irrigated 27-gauge retractable needle-tipped electrode [10]. This allows radiofrequency ablation to be delivered directly inside the myocardial wall, overcoming the issue of intramural lesion delivery. In addition, refined mapping can be performed by intramyocardial pacing and recording.
...to non-RF ablation.
What if RF is not the future? RF remains the standard energy source in ablation. However, different ablation modalities can provide advantages in certain clinical scenarios. Chemical ablation with alcohol injection, although far from novel, remains an alternative modality in ablation for arrhythmias.
Alcohol infusion in the Vein of Marshall made it possible to create a conduction block more easily in the mitral isthmus (classically difficult to ablate with radiofrequency energy) and improves the prognosis of persistent AF ablation, especially by reducing the risk of recurrence in the form of perimitral flutter for selected patients [11]. The same principles exist in the ventricles to access intramyocardial circuits. Transmural lesions can be achieved both from the arterial and the venous coronary circulation.
Recently, another game changer has come into the portfolio of available tools. Irreversible electroporation can be used as a non-thermal energy source to ablate tissue. Cardiac catheter ablation by irreversible electroporation may be a safe and effective alternative for thermal ablation techniques such as RF or cryoablation [12]. Electroporation can be achieved with various modalities: direct current, alternating current, pulsed direct current, or any combination of these. Experimental cardiac and noncardiac studies have demonstrated tissue specificity with survival of arteries and nerves in large lesions. In addition, data from porcine trials suggest that application inside a pulmonary vein does not lead to pulmonary vein stenosis and that the oesophagus is remarkably insensitive to electroporation [13]. Therefore, irreversible electroporation is a very promising technique for cardiac catheter ablation and especially for electrical pulmonary vein isolation. The proof will be in the pudding.
Conclusion
In this review, we have seen how advances developed in ablative techniques relating to complex arrhythmia mapping, RF application and deep circuit tracking. When you look back 10 years, cardiac electrophysiologists look more like NASA engineers than nerdy coders. These recent techniques allow for more precise, safer and faster ablations and many advances are still to come. Just as the word nerd, while originally pejorative, has been taken to be a source of pride, so electrophysiologists have gone from being like Cinderella, locked away in a dark room, to become the stars of cardiology.
Take Home Messages
- In the last decade, the techniques of ablation have drastically changed.
- The complexity of reentrant arrhythmias have been mastered since the rise of HD mapping
- Smart algorithms that deliver RF (taking into consideration multiple parametrics: power, force, duration, stability, impedance, etc..) are used for homogeneous lesions to achieve better outcomes.
- It was the imagination of those performing ablations that gave birth to the new techniques (i.e., ethanol, bipolar, electroporation).
- Although elegant and promising clinical trials exist, more trials are still needed to demonstrate long-term benefits.
