

















Abbreviations
ACM: arrhythmogenic cardiomyopathy
AOCA: anomalous origin of coronary arteries
BP: blood pressure
CAD: coronary artery disease
CACS: coronary artery calcium scoring
CHD: congenital heart disease
CTCA: computed tomography coronary angiography
CVD: cardiovascular disease
ECG: electrocardiogram
HCM: hypertrophic cardiomyopathy
MVP: mitral valve prolapse
PA: physical activity
SCA: sudden cardiac arrest
SCD: sudden cardiac death
SVT: supraventricular tachycardia
Introduction
Despite the importance of sports, exercise may paradoxically trigger sudden cardiac arrest (SCA) in individuals with cardiovascular disease (CVD), particularly those who were previously sedentary or have advanced CVD [1].
At the same time, sudden cardiac death (SCD) is the main cause of sports- and exercise-related mortality in athletes [2].
CV safety and avoiding of fatal events during the practice of sports is imperative and has become a common goal in many sports institutes [3].
Screening strategies should be tailored to the specific population groups and the different cardiac disorders [4].
Special emphasis should be applied to high-risk groups during their pre-participation screening as well as during their follow-up.
Prevention of SCD requires certain eligibility conditions before practising sport.
In addition to pre-participation screening, special equipment should be available in clubs for prevention of SCD and management of SCA.
Definition
SCA in athletes could be defined as sudden collapse due to any cardiac aetiology in which cardiopulmonary resuscitation (CPR) and/or direct current (DC) shock is applied to an athlete regardless of the survival outcome [2].
SCD is defined as a sudden unexplained death due to any cardiac aetiology, or sudden death with a structurally normal heart post mortem with no other explanation for death and a history suggesting cardiac-related death [2].
SCD in athletes can be categorised according to the time of occurrence as that occurring during the exercise, within the first hour post exercise, or between 1 and 24 hours post exercise. The practice of sport at the time of SCD can be further classified as occurring during ordinary training or during competitive games [5].
Incidence of SCD in athletes
Current reports about the incidence of SCD in competitive athletes range from almost 1 in a million to 1 in 5,000 athletes per year [2,6].
The incidence of cardiac arrest increases acutely with vigorous exercise, especially in those who do not exercise regularly.
Previous reports show that 56-80% of SCA in young athletes occurs during exercise [2]. Some variables including sex, race and type of sport may increase the risk of SCA [2,6]. Relative risk increases in male athletes compared to female athletes, with a range from 3:1 to 9:1 (male:female) [2]. Black athletes also have a higher risk than white athletes (1 in 21,000 vs 1 in 68,000) [2].
Genetic and congenital structural cardiac disorders are usually the cause of SCD in young athletes [2,7]. However, in older athletes >35 years of age, SCD is due mainly to atherosclerotic coronary artery disease (CAD) in most cases, with increased risk with vigorous exercise. Athletes with little or no background in systematic training have the greatest risk [4].
Pre-participation screening programmes
A systematic pre-participation evaluation programme can significantly decrease SCD among athletes via identification of those with a cardiac disorder before licensing for sport practice, exercise modification and disease-related intervention [8]. For competitive or professional athletes, personal history, physical examination and a resting 12-lead electrocardiogram (ECG) are recommended [9].
Pre-participation screening allows application of appropriate measures to prevent SCD in athletes with clinically silent CVD through lifestyle modification, including restriction of competitive sports activity (if necessary), but also by prophylactic treatment with drugs and implantable defibrillators.
Screening for cardiovascular disease in young athletes
Pre-participation screening modalities in young athletes present specific challenges and limitations.
Despite low sensitivity, pre-participation history questionnaires show a high positive response rate. However, CV screening using ECG outperforms history and physical examination [10].
There are insufficient data to recommend an echocardiogram for routine screening without evidence of CV disorder warranting echocardiography performance.
Screening for cardiovascular disease in older athletes
The recommendations and evidence base for CV screening in athletes >35 years of age are limited. CV screening in senior athletes must be directed to atherosclerotic CAD.
ECG screening can uncover some latent cardiomyopathies as well as electrical disorders in older athletes. In addition, risk factor assessment for CVD may identify higher-risk individuals who need additional screening tests.
Despite CAD being the main aetiology of SCD in older athletes, routine screening for ischaemia with stress testing in asymptomatic individuals is not recommended. However, exercise ECG should be reserved for symptomatic or high-risk athletes based on the ESC Systematic Coronary Risk Evaluation (SCORE) system [11].
An exercise ECG test may also be important to evaluate the blood pressure (BP) response to exercise, the occurrence of exercise-induced arrhythmias, and to assess the functional capacity needed for exercise training. Exercise testing may also be helpful in the evaluation of CV functional capacity in elderly individuals who have recently engaged in moderate or severe exercise.
Prevention of scd in special populations
Anomalous origin of coronary arteries (AOCA)
SCD may result from ischaemic attacks due to the compression of the anomalous vessel coursing between the aorta and the pulmonary artery during exercise and/or the proximal intramural course of the anomalous coronary [12]. This frequent ischaemic episode may precipitate myocardial fibrosis and consequent ventricular arrhythmias during exercise.
Multislice contrast-enhanced computed tomography (CT), computed tomography coronary angiography (CCTA), or cardiac magnetic resonance (CMR) are the mainstays of diagnosis and should be considered together with an exercise test to identify high-risk individuals with AOCA. Participation in sports, more than low-intensity skill sports, is discouraged regardless of symptoms.
Valvular heart disease:
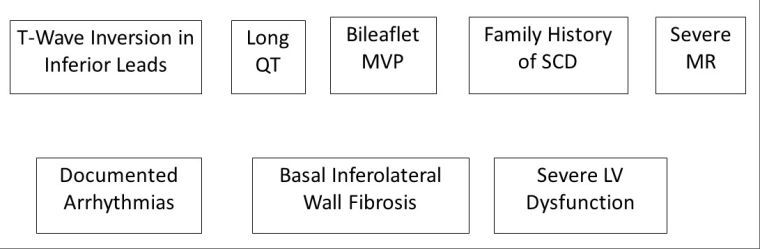
Mitral valve prolapse (MVP)
High-risk features for SCD are presented in Figure 1.
An exercise test and 24-hour Holter ECG should be considered in the evaluation of individuals with MVP. Individuals with high-risk features where myocardial fibrosis affecting the infero-basal wall is suspected should undergo a CMR imaging scan. Symptomatic patients with MVP and any of the high-risk features should not participate in recreational or competitive sports.
Hypertrophic cardiomyopathy (HCM)
Exercise carries a high risk of SCD/SCA for individuals with HCM. Consistently, all athletes with HCM have been recommended not to participate in competitive sports [9]. In addition, certain sports may carry a higher risk for SCD, such as highly dynamic, start-stop sports like basketball and football [2].
More recently, a more liberal approach to sports practice has been accepted in some individuals after careful evaluation [14]. This applies to amateur sports or leisure-time exercise to maintain physical and psychological well-being.
The baseline evaluation should include a detailed personal and family history, assessment of the clinical severity of HCM, and the presence of any other risk factors for SCD/SCA.
Individuals with a history of SCA or syncope and individuals with exercise-induced symptoms are recommended to engage in low-intensity recreational sports only. Holter ECG monitoring for 48 hours is recommended to detect ventricular and supraventricular arrhythmias.
Echocardiography should be used for risk stratification for SCD by assessing the following indices: (i) left ventricular (LV) wall thickness; (ii) LV outflow tract (LVOT) gradient at rest, during the Valsalva manoeuvre, on standing suddenly, and after light exercise; and (iii) left atrial diameter [15].
CMR imaging may be considered for confirming the diagnosis and for risk stratification in HCM.
Individuals with HCM who exercise on a regular basis should be followed up annually or biannually according to their vulnerability for exercise-related SCD. Follow-up should consider disease progression and the development of new symptoms that prompt interruption of exercise and re-evaluation.
Arrhythmogenic cardiomyopathy (ACM)
Regular and high-intensity exercise carries worse outcomes.
Competitive sports increase the risk of ventricular tachyarrhythmias or death twofold.
The baseline evaluation should include a detailed history of symptoms and family history of a similar disorder or SCD, clinical assessment of the severity of the ACM, and the presence of any traditional risk factors for SCD/SCA.
An ECG is important for risk stratification in ACM. The presence of extensive T-wave inversion in ≥3 precordial leads or T-wave inversion in two of the three inferior leads presents some additional risk for SCD/SCA [16].
Ambulatory ECG monitoring should include exercise periods to detect ventricular arrhythmias.
The presence of non-sustained ventricular tachycardia or high burden of ventricular ectopy (≥1,000/24 h), even in asymptomatic individuals, increases the risk of fatal arrhythmias [17].
Risk stratification for SCD in ACM includes echocardiography or CMR imaging assessment of the level of right ventricular (RV) and LV involvement.
Exercise testing should be part of the routine assessment of every individual with ACM who wants to exercise but away from “hot phases”, to assess the functional capacity and risk stratification.
An annual or biannual follow-up is recommended for ACM individuals who exercise on a regular basis according to SCD risk.
Dilated cardiomyopathy
Participation in high-intensity exercise as well as competitive sports may be allowed in asymptomatic individuals who fulfil certain low-risk criteria (Table 1).
Table 1. Low-risk criteria for SCD in dilated cardiomyopathy. Adapted from [4] (Pelliccia A, et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease: The Task Force on sports cardiology and exercise in patients with cardiovascular disease of the European Society of Cardiology (ESC). Eur Heart J. 2020;42:17-96) by permission of Oxford University Press on behalf of the European Society of Cardiology.
Sports Cardiology and exercise in patients with cardiovascular disease Guidelines
|
Low risk criteria for SCD in dilated cardiomyopathy
|
|---|
|
|
|
|
|
Myocarditis
A comprehensive evaluation after complete recovery to assess the risk of exercise-related SCD should include imaging studies, exercise stress test, and Holter monitoring.
Repeated evaluation including measurement of troponin and inflammatory biomarkers, echocardiography, and prolonged ECG monitoring should be carried out. Individuals without evidence of ongoing myocarditis should undergo an exercise stress test. CMR imaging should be repeated if myocardial oedema or late gadolinium enhancement (LGE) was present during the acute illness.
Asymptomatic individuals could return to sport when the troponin and inflammatory biomarkers return to normal, LV systolic function normalises, myocardial fibrosis on CMR disappears, and complex arrhythmias during exercise also disappear.
Pre-excitation and supraventricular tachycardia (SVT)
Pre-excitation may be associated with SCD; therefore, athletes with paroxysmal SVT should stop exercise once palpitations occur. The responsible physician should educate individuals with SVT on how to perform vagal manoeuvres safely to terminate the arrhythmia. Exercise may be resumed after arrhythmia termination. Beta-blockers or calcium channel blockers could be used as a prophylactic treatment.
In competitive athletes with asymptomatic pre-excitation an electrophysiological (EP) study is warranted to evaluate the risk of SCD.
In the case of high-risk individuals, ablation of the accessory pathway is recommended.
Long QT syndrome (LQTS)
Symptomatic athletes are forbidden from engaging in competitive sports.
Special categories such as LQT1 should not engage in diving into cold water since this is associated with an increased risk of arrhythmias. Preventive measures include avoidance of QT-prolonging drugs, dehydration, and electrolyte imbalance. Beta-blocker drugs could be used effectively in LQT1.
Individuals who present with syncope or SCA despite beta-blocker therapy should be referred for an implantable cardioverter defibrillator (ICD).
Brugada syndrome
Arrhythmic syncope or SCA during exercise warrants ICD implantation in athletes. An EP study may play a role in detecting individuals at risk of SCD.
Complex congenital heart disease (CHD)
Many complex CHD patients with the highest risk of SCD have reduced exercise capacity and cannot usually practise a significant athletic activity. However, some groups, e.g., post tetralogy of Fallot repair, carry a risk of SCD but can still compete in low-intensity sport. SCD in CHD patients under 35 years was due to a presumed arrhythmia in 87% of cases in a large population-based study [18].
Pre-participation athletic screening including an ECG and echocardiography is important.
Pre-participation screening modalities
Pre-participation cardiovascular evaluation is recommended mainly by means of history (personal and family history) and physical examination alone. However, a 12-lead ECG improves the sensitivity of the screening process through early detection of CV disorders with specific ECG changes, such as cardiomyopathies, pre-excitation syndromes, and channelopathies [18]. These ECG changes are found in approximately two thirds of young competitive athletes with SCD.
Some authors consider ECG as a poor screening test in athletes, because of high false-positive results [20].
Role of ECG exercise test
Exercise testing is indicated in athletes during a pre-participation screening for the following purposes:
- To diagnose CAD
- Assess the blood pressure response to exercise
- Detect the exercise-induced arrhythmias
- Evaluate symptoms occurring during physical activity
- Assess the physical fitness and functional capacity relative to training and type of sport
- For diagnostic or therapeutic approach in some conditions, e.g., LQTS
Role of ambulatory ECG monitoring
The most important indications for ambulatory ECG monitoring are unexplained syncope and palpitations during or after exercise. It may also be used in the documentation of bradyarrhythmias or quantification of the burden of premature ventricular beats related to exercise. Holter ECG monitoring is considered also in specific cases such as LQTS.
Role of imaging modalities
Imaging modalities have been integrated in the pre-participation screening of athletes who are suspected of having a cardiac disorder [17]. Transthoracic echocardiography and CMR will detect the majority of cardiomyopathies. CTCA and CMR are the non-invasive modalities of choice for coronary artery anomalies. Coronary artery calcium scoring (CACS), CTCA, and stress imaging are reserved for the evaluation of athletes with suspected atheromatous CAD.
Criteria for positive cases in pre-participation screening
Some criteria are considered positive and risk factors for SCD during initial screening and warrant further investigation before disqualification from competitive sport [21].
These criteria include the following.
Family history
- Close relative(s) with premature MI or SCD at <50 years
- Family history of cardiomyopathy, CAD, Marfan syndrome, LQTS, severe arrhythmias, or other disabling cardiovascular diseases.
Personal history
- Syncope or pre-syncope
- Exertional chest pain or shortness of breath or fatigue out of proportion to the degree of physical effort
- Palpitations or irregular heartbeat
Physical examination
- Musculoskeletal and ocular features suggestive of Marfan syndrome
- Diminished and delayed femoral artery pulses
- Mid- or end-systolic clicks
- Abnormal second heart sound (single or widely split and fixed with respiration)
- Heart murmurs (systolic grade ≥2/6 and any diastolic)
- Brachial blood pressure ≥140/90 mmHg on more than one reading
Electrocardiogram
- Left and/or right atrial enlargement
- Frontal-plane QRS axis deviation
- Increased voltage
- Abnormal Q-waves
- Right or left bundle branch block
- ST-segment depression or T-wave flattening or inversion in ≥2 leads
- Prolonged corrected QT interval
- Premature ventricular beats or more severe ventricular arrhythmia
- Supraventricular tachycardia, atrial flutter, or fibrillation
- Ventricular pre-excitation
- First-degree, second-degree, or third-degree atrioventricular block
Other preventive strategies
The screening ability to detect young competitive athletes with either atherosclerotic or congenital coronary lesions is limited by the absence of baseline ECG changes in many cases with premature disease [18].
Moreover, SCD during sports may occur due to non-penetrating chest injury (commotio cordis) which cannot be prevented by screening. This requires the implementation of an additional prevention strategy based on early external defibrillation of SCA. The presence of a free-standing automated external defibrillator (AED) at sporting events is a valuable preventive measure for SCD in conditions undetected by screening.
However, the availability of an AED should neither replace a pre-participation evaluation programme nor justify engagement of high-risk athletes in competitive sports.
Conclusion
SCD can occur in athletes during competitive sports. The aetiology of SCD differs according to the age of athletes, associated cardiac disorder and type of sport. A pre-participation screening programme should be applied to all athletes before qualification. Baseline history and physical examination should be carried out as an essential part of screening. Other different modalities should be applied if needed according to different situations. The presence of positive criteria indicating a high risk for SCD requires disqualification or the modification of exercise practice.
