















Abbreviations
ACL adenosine triphosphate citrate lyase
ApoB apolipoprotein B
ASCVD atherosclerotic cardiovascular disease
BA bempedoic acid
BAS bile acid sequestrants
BP blood pressure
CETP cholesteryl ester transfer protein
CHD coronary heart disease
CV cardiovascular
CVD cardiovascular disease
CVE cardiovascular event
DM diabetes mellitus
DPP-4is dipeptidyl peptidase-4 inhibitors
EPA eicosapentaenoic acid
GLP-1 RA glucagon-like peptide-1 receptor agonists
GFR glomerular filtration rate
HDL high-density lipoprotein
hsCRP high-sensitivity C-reactive protein
IPE icosapent ethyl
ITBs incretin-based therapies
LDL low-density lipoprotein
LpL lipoprotein lipase
MACE major adverse cardiovascular events
mRNA messenger ribonucleic acid
NAFLD non-alcoholic fatty liver disease
non-HDL-C non-high-density lipoprotein cholesterol
NPC1L1 Niemann-Pick C1-Like 1
PCSK9 proprotein convertase subtilisin/kexin type 9
PPAR-α proliferator-activated receptor α
RNA ribonucleic acid
sd LDL small, dense low-density lipoprotein
SGLT2is sodium-glucose cotransporter 2 inhibitors
SPPARM-α selective PPAR-α modulator
T1DM type 1 diabetes mellitus
T2DM type 2 diabetes mellitus
TRG triglyceride
VLDL very low-density lipoprotein
Introduction
Cardiovascular disease is the leading cause of morbidity and mortality among people living with diabetes, and diabetes mellitus (DM) is one of the leading causes of premature atherosclerosis in all genders [1].
DM itself is an independent risk factor for cardiovascular disease (CVD) and is associated with a higher risk of CVD, even more so in women.
Dyslipidaemia is very common in type 2 diabetes mellitus (T2DM), affecting around 72% to 85% of patients, with a more atherogenic lipid profile that includes hypertriglyceridaemia, high levels of apolipoprotein B (ApoB), non-high-density lipoprotein (HDL), small, dense low-density lipoprotein (LDL), and low HDL. Understanding diabetic dyslipidaemia is important as it can occur and bring on cardiovascular (CV) events before the diagnosis of diabetes.
Emerging evidence suggests considering lipid-lowering therapies more often in younger patients with type 1 diabetes (T1DM) and in those with T2DM. As younger patients with T2DM and T1DM lose the greatest number of years of life expectancy due to diabetes, it is important that such patients should be offered medications to prevent it earlier in their lives.
Some people who are strongly resistant to insulin develop DM2 in their youth because of extreme obesity or a genetic cause. In these cases, the lifetime risk of CVD is astronomic.
Cardiovascular risk in diabetes is multifactorial, with obesity, hypertension, and specific dyslipidaemia frequently coexisting. Recent studies suggest that much of the excess of CVD incidence in diabetes is because of inadequate treatment of lipids and blood pressure (BP).
Being aware of the therapeutic benefit of classes of lipid-lowering therapies, which are available, is of paramount importance.
Statins are considered first-line treatments for many people with T2DM, even at diagnosis, without other apparent risk factors. Concerning those patients with multiple risk factors for CVD, high-dose statin is recommended [2,3].
Pathophysiology of diabetic dyslipidaemia
The most common lipid abnormalities are hypertriglyceridaemia associated with increased concentrations of triglyceride (TRG)-rich lipoproteins, mainly those consisting of large very-low-density lipoprotein (VLDL1) and their remnants. Decreased HDL cholesterol (mainly due to decreased HDL2 particles secondary to an increased rate of HDL catabolism) and normal or slightly increased LDL cholesterol levels with a predominance of atherogenic small, dense LDL (sd LDL) particles are the greater contributors to atherogenic disease. Such particles cannot be detected in routine measurements of LDL. Increased glycation and oxidation of these particles also occurs. These alterations are related to CVD risk and are the major treatment target in diabetic patients [4,5].
Insulin plays an important role in regulating lipid metabolism. It acts on the liver by inhibiting the production of VLDL, increases LDL receptors, and reduces free fatty acids and the production of ApoB. In addition, it inhibits the hormone-sensitive lipase in adipocytes, activates lipoprotein lipase in the circulation and increases the catabolism of chylomicron remnants.
Lipid abnormalities are quantitative, qualitative, and kinetic in nature [4,5] (Table 1).
Table 1. Major changes in lipoprotein metabolism in T2DM.
|
Lipoprotein |
Quantitative changes |
Qualitative changes |
Kinetic/metabolic changes |
|
LDL |
No change or slight increase |
Higher proportion of small dense particles |
Decreased catabolism |
|
HDL |
Decreased plasma concentration |
Glycation |
Increased catabolism |
|
VLDL |
Increased plasma concentration |
Higher proportion of larger particles (VLDL1) |
Increased production |
Some patients have atherosclerotic disease before the diagnosis of diabetes.
As LDL levels may remain within the normal range, the lipid measures used in clinical practice do not always reveal the malignant nature of diabetic dyslipidaemia. It may be better revealed by non-HDL levels.
Treatment targets
The cornerstone of treatment is lipid-lowering drugs. The guidelines vary in their recommendations and use different markers. It is important to risk stratify the patient to determine the therapeutic target of LDL. The targets of lipid-lowering therapy in DM do not have a consensus among medical societies. Most recently, DM has been considered a high-risk condition: risk enhancers of this disease are diabetes duration of >10 years in T2DM and >20 years duration for T1DM, albuminuria >30 mg/G creatinine, an estimated GFR <60 mL/min /1.73 m2, retinopathy, neuropathy and an ankle-brachial index (ABI) <0.9. Hypertension, dyslipidaemia, abdominal obesity, and non-alcoholic fatty liver disease (NAFLD) commonly coexist with T2DM and further aggravate the risk of CVD. These conditions indicate statin therapy, a keystone treatment in diabetic dyslipidaemia [6,7].
Treatment of diabetic dyslipidaemia
The treatment of diabetic dyslipidaemia can be divided into two phases: non-pharmacological and pharmacological.
Non-pharmacological treatment includes medical nutrition therapy with a focus on the reduction of saturated and trans fat intake and increases in dietary fibre, weight loss, including bariatric surgery (if needed) and physical activity.
Pharmacotherapy
Weight loss has been shown to improve multiple risk factors, such as haemoglobin A1C and blood pressure; however, the “Look AHEAD” study did not show improvement in CV events after long-term weight loss with intensive lifestyle change, indicating the need for pharmacotherapy to reduce atherosclerotic cardiovascular disease (ASCVD).
The old drugs used to treat diabetic dyslipidaemia include statins, cholesterol absorption inhibitors, niacin, fibrates, bile acid sequestrants (BAS), and omega-3 free fatty acids. A relatively novel agent proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor and other agents still on the horizon (such as icosapent ethyl [IPE], bempedoic acid [BA], and inclisiran) are options to manage this important risk factor [1].
Diabetic dyslipidaemia should be treated with statins. However, some patients do not reach the established therapeutic target for LDL and are candidates for potential combination therapy (Figure 1).
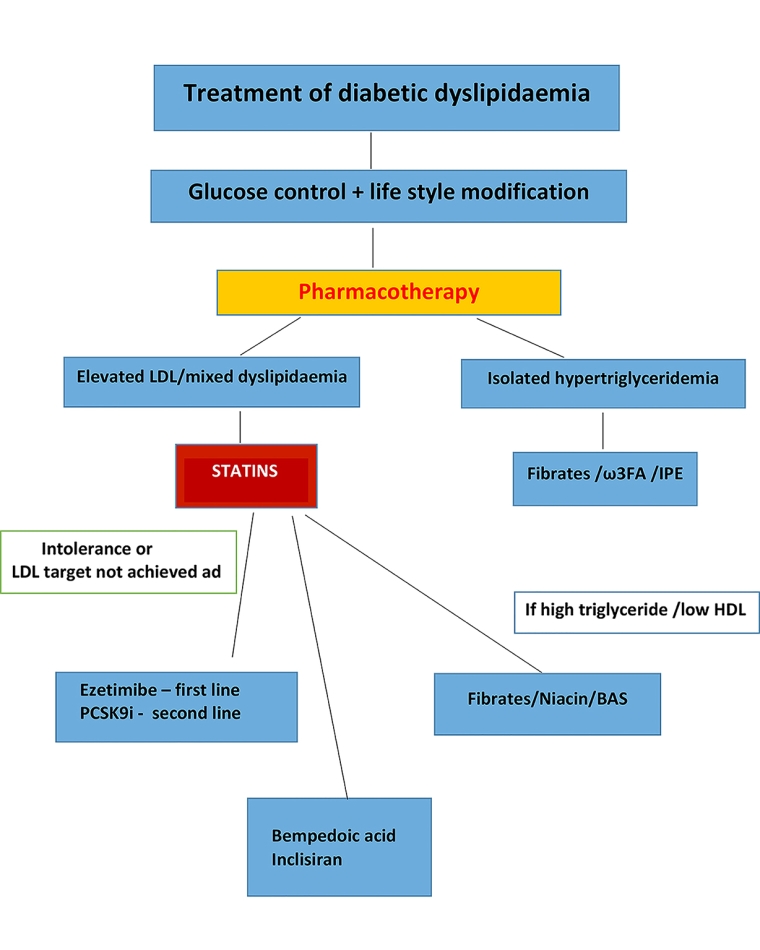
Figure 1. Treatment algorithm for diabetic dyslipidaemia. Statins are the cornerstone of the treatment. Combination therapies may be considered in patients at very high risk.
Statins
Statins competitively inhibit 3-hydroxymethylglutaryl coenzyme A, which is a rate-limiting step in the synthesis of cholesterol in the liver. They are considered first-line treatments for patients with T2DM, even at diagnosis. For these reasons, statins have been associated with significant reductions in LDL concentration as well as CVD risk reduction in both primary and secondary prevention in patients with DM. This notion is supported by many randomised controlled trials.
It should be considered that individuals with T2DM with additional CV risk factors receive statin therapy regardless of their baseline LDL levels [8].
According to guidelines, all DM patients should be treated with statins, if tolerated, with different LDL goals based on the type of DM, CV risk factors, and complications.
Statins reduce cholesterol deposits, increase expression of LDL receptors in the liver and enhance endocytosis of the circulating LDL. They also have pleiotropic effects - reduction of high-sensitivity C-reactive protein (hsCRP) and other markers of inflammation that help to stabilise plaque, improve endothelial function, and decrease vascular inflammation and oxidative stress [6,9].
Statins are divided into:
High-intensity – these statins decrease LDL by 50% or more (atorvastatin 40-80 mg, rosuvastatin 20-40 mg).
Moderate-intensity – these statins decrease LDL by approximately 30-50% (atorvastatin 10-20 mg, rosuvastatin 5-10 mg, simvastatin 20-40 mg, pravastatin 40 mg, lovastatin 40 mg, fluvastatin 80 mg, pitavastatin 2-4 mg).
Low-intensity – these statins decrease LDL by <30% (simvastatin 10 mg, pravastatin 10-20 mg, lovastatin 20 mg, fluvastatin 20-40 mg, pitavastatin 1 mg).
Many trials have shown a reduction in CV events with statin use. The Heart Protection Study reported a 22% reduction of events including stroke [10].
A meta-analysis of 14 randomised clinical trials including over 18,000 patients with T2DM demonstrated, during an average follow up of 4.3 years, that statin therapy reduced CVE by 21% and vascular mortality by 13% for every 39 mg/dL reduction in LDL [11]. It is important to note that the benefits of using statins in diabetic patients were independent of LDL and lipid values.
Statins are generally well tolerated. The most common side effect is myalgia. Necrotising autoimmune myopathy and rhabdomyolysis are rare. However, caution is needed in elderly patients, especially those with chronic kidney disease or patients with untreated clinical or subclinical hypothyroidism, and those receiving drugs that interact with statins. Statins can also cause new-onset diabetes, but the risk is very low compared with the statin-induced decrease in CVD events [6,8]. It is important to certify that intolerance to statins is true to avoid unnecessary suspension of the drug [12,13].
Cholesterol absorption inhibitors – ezetimibe
Ezetimibe acts by inhibiting intestinal absorption of cholesterol binding to sterol transporter Niemann-Pick C1-Like 1 (NPC1L1), ultimately causing a reduction in LDL. Ezetimibe appears to increase insulin sensitivity in patients with insulin resistance. It is particularly efficacious in patients with DM, reducing LDL by 24%. There is an intensification of LDL reduction when ezetimibe is added to statin therapy.
The IMPROVE-IT trial showed that ezetimibe add-on therapy to simvastatin is particularly beneficial for diabetic patients, with a relative risk reduction in CVE of 15% and an absolute risk reduction of 5.5%. A meta-analysis (n=109,244) showed that an ezetimibe/statin combination leads to a significant reduction of CV events in patients with high CVD risk [7,8,14].
Ezetimibe associated with statins is indicated for diabetic patients with suboptimal lipid levels despite maximal dose of statin therapy, individuals unable to tolerate maximum statin doses or as monotherapy in patients who are statin intolerant [9,12].
Niacin
Niacin is a potent drug to increase HDL and to reduce LDL and TRG moderately. In addition, it can lower lipoprotein(a) levels by 25%. However, its benefits have not been proven effective in reducing CV events. In practice, the use of niacin is limited by its side effects: at the standard dose, 80% of users describe flushing, and another 20% complain of pruritus, paraesthesia, and nausea.
The AIM-HIGH trial showed no clinical benefit despite significant improvements in HDL and TRG levels. Thus, the combination of statin with niacin in diabetic subjects has no clinical benefit and should be avoided [8,15].
Fibrates
Fibrates reduce serum TRG levels and increase HDL levels by means of activation of peroxisome proliferator-activated receptor α (PPAR-α) and promote a moderate reduction in LDL. Fenofibrate reduces TRG concentration by 30-50%. Its effects are seen in high-risk diabetic patients with high triglyceride levels.
The FIELD study showed that fenofibrate should be considered in individuals with hypertriglyceridaemia and low HDL and high CV risk but should not be considered a substitute for statins. A meta-analysis with 45,058 participants showed that fibrates reduce the relative risk of major events by 10% and the risk of coronary events by 13%.
Fibrates are metabolised in the kidney and should be avoided or used with caution in patients with kidney disease [12].
Pemafibrate is a selective PPAR-α modulator (SPPARM-α), a newer, more potent fibrate. It is metabolised in the liver and excreted into the bile, so it can be used in patients with kidney dysfunction. The ongoing PROMINENT trial is evaluating the effect of pemafibrate in reducing CV events [9].
Bile acid sequestrants (BAS)
BAS bind to bile acids in the intestinal lumen interrupting the enterohepatic circulation of bile acids, reducing the level of LDL by up to 30%.
Cholestyramine, colestipol, and colesevelam are commonly used BAS. Historically, they have been used when statins are not tolerated, in women of childbearing age and in children. Their side effects such as constipation, cholelithiasis, and hypertriglyceridaemia limit their use. Colesevelam has a lower incidence of these side effects and the benefit of improving HbA1c in patients with inadequately controlled diabetes.
BAS are considered second-line therapy for lowering LDL and are used in combination therapy [15,16].
Icosapent ethyl (IPE)
Omega-3 free fatty acids are used as a complementary therapy to reduce the level of triglycerides, but their effects on other lipoproteins are trivial. High doses (3-5 g) of the formulation eicosapentaenoic acid (EPA) + docosahexaenoic acid are necessary to show any CV benefit.
Icosapent ethyl is a highly purified EPA ethyl ester. It acts on PPAR expressed on adipocytes and inflammatory cells to reduce levels of TRG, increase insulin sensitivity, and regulate the inflammatory cascade.
Recently, the REDUCE IT trial showed that the primary endpoint of major adverse CV events (MACE) was significantly lower in the group treated with IPE versus placebo, p<0.001, but an increase in hospitalisation for atrial fibrillation or flutter was observed.
IPE emerges as an option adjunct to statins to treat patients with ASCVD and high TRG levels [1,6].
Bempedoic acid (BA)
Bempedoic acid decreases LDL level through competitive inhibition of adenosine triphosphate citrate lyase (ACL), an enzyme responsible for catalysing the production of acetyl coenzyme A, an integral substrate in the cholesterol synthesis pathway in the liver. It acts in a similar way to statins, upregulating the expression of the hepatic LDL receptor, increasing the clearance of circulating LDL [17]. Randomised trials have shown an LDL decrease from 18% to 28% when BA can be used as monotherapy or added to statin. It requires activation by an enzyme present in the liver, not in the muscles, decreasing the risks of muscle-related adverse effects, but there is an increase in uric acid and gout can occur.
A meta-analysis of 7 randomised trials concluded that BA is a valuable option for patients with statin intolerance and a high CV risk, not reaching the LDL target, despite a maximally tolerated lipid-lowering treatment, including both statin and ezetimibe.
Inclisiran
Inclisiran is a synthetic small interfering ribonucleic acid (RNA) that leads to the degradation of PCSK9-specific messenger RNA (mRNA) in the liver. It is a long-acting agent (1 to 2 times a year) that decreases PCSK9 production by the liver. It results in a reduction of LDL levels of >50%.
Inclisiran differs from other PCSK9 inhibitors due to its longer duration of action and acts at an intracellular level within hepatocytes, as opposed to the plasma level. It yields a rapid, significant and prolonged reduction in LDL levels, improves atherogenic lipids and lipoprotein profiles, and is safe and well tolerated. Like other PCSK9 inhibitors, the cost limits its use [1,18].
The use of twice a year therapy has the potential to improve adherence and achieve the most complete LDL goal [18].
Type 1 diabetes mellitus (T1DM)
The exposure of patients with DM1 to hyperglycaemia is of paramount importance in the development of CVD. Duration of diabetes is important. These patients develop the disease early in their lives, during childhood. The pattern the disease shows is more atherosclerotic, driven by hyperglycaemia and ensuing early renal damage. Furthermore, even minimal evidence of nephropathy greatly increases the risk of CVD in T1DM. It may be prudent to consider statins for the majority of patients with T1DM above the age of 30 [2,3].
Antidiabetic drugs
Clinical studies have highlighted the effect of novel antidiabetic drugs beyond glucose lowering - reduction in body weight, blood pressure, lipids, inflammatory markers, oxidative stress, endothelial dysfunction and subclinical atherosclerosis. Incretin-based therapies (IBTs), including glucagon-like peptide-1 receptor agonists (GLP-1RA), dipeptidyl peptidase-4 inhibitors (DPP-4is), sodium/glucose cotransporter 2 inhibitors (SGLT2is), have beneficial effects, reducing CV events [3,9] (Table 2).
Table 2. Effect of antidiabetic drugs on lipoproteins.
|
DRUG
|
TOTAL CHOLESTEROL
|
LDL
|
HDL
|
TRG |
|---|---|---|---|---|
| Metformin | - /0 |
- |
0/+ | - /0 |
|
DPP-4 inhibitors |
||||
|
Sitagliptin |
0 |
0 |
0/+ | 0 |
|
Vildagliptin |
0 |
0 |
0/+ | 0 |
|
Saxagliptin |
0 |
0 |
0 | 0 |
|
Linagliptin |
0 |
0 |
0 | 0 |
|
GLP1 analogues |
||||
|
Liraglutide |
0 |
0 |
0 | - |
| Exenatide | -/0 |
0/+ |
0/+ | - |
|
SGLT2 inhibitors |
||||
|
Empaglifozin |
0/+ |
0/+ |
0/+ | - |
|
Dapaglifozin |
0/+ |
0/+ |
0/+ | -/0 |
|
Canaglifozin |
+ |
+ |
+ | + |
|
Insulin |
-/0 |
- |
0/+ | - |
DPP-4: dipeptidyl peptidase-4; GLP1: glucagon-like peptide-1; SGLT2: sodium/glucose cotransporter 2; LDL: low-density lipoprotein; HDL: high-density lipoprotein; TRG: triglyceride
0: no effect +: increase -: decrease
0/+: no effect or increase -/0: no effect or decrease
Conclusion
Diabetic dyslipidaemia represents a high risk for developing ASCVD. All of its three components, namely hypertriglyceridaemia, low HDL and high sdLDL levels, are metabolically linked, with hypertriglyceridaemia being the dominant feature. Effectively managing diabetic dyslipidaemia is significant in reducing the risk of CVD.
The risk of CVD can be underestimated in diabetes with risk mechanisms based on the populations of survivors, which are not applicable to younger people.
Emerging evidence suggests the need to consider lipid-lowering therapies more frequently in younger patients with T1DM and T2DM.
Statins should always be considered first-line therapy. In general, statins can be administered to all diabetic patients when LDL is above 100 mg/dL, starting with a moderately potent statin and continuous monitoring of LDL.
Ezetimibe in combination with statins can result in an incremental reduction in LDL levels and improve cardiovascular outcomes further. Fibrates have a role in patients with high TRG and low HDL, and fenofibrate should also be considered in patients with T2DM and retinopathy. Finally, PCSK9 inhibitors are a new class of lipid-lowering drugs that can be integrated into the treatment of individuals with diabetes and dyslipidaemia. They can be used in addition to statins, ezetimibe, and fibrates.
It is important to know that treating lipid abnormalities has the potential to reduce CV events by more than 50%.
