















Introduction
The number of endovascular aortic repairs (EVARs) has increased significantly during the first two decades of the new century due to less invasive treatment with a marked improvement in perioperative morbidity, mortality and recovery compared with open surgery. Thanks to this, in most developed countries, elective treatment of abdominal aortic aneurysm (AAA) is mostly performed EVAR. However, some recent studies have shown that the early survival benefit of EVAR decreases or is even lost over time, with EVAR carrying a higher risk of rupture and secondary intervention than open repair (OR) in the long term [1]. Due to this, an OR of AAA is still very important and should not be forgotten in the endovascular era. In the following article, the indications and contraindications for both open as well as endovascular repair of different AAAs will be considered.
Degenerative AAA
One of the most common forms of AAA is degenerative AAA. The main question regarding the treatment options in cases of degenerative AAA with suitable anatomy is probably, “Should young patients with good risk factors be treated with EVAR?” [2]. In my opinion, patient motivation and surgical experience should not be the main reasons for EVAR in those patients. At the moment, there is no evidence in the recent literature to support EVAR as the first-line therapy in patients younger than 60 or even 70 years old [2]. As in the majority of previous studies and articles, the most recently published meta-analysis found significantly lower odds of 30-day (OR 0.36, 95% CI: 0.20-0.66) and in-hospital mortality with EVAR (OR -0.03; 95% CI: -0.04 to -0.02) [3]. However, my clinic’s experience confirms that high hospital and surgical volumes, together with careful preoperative selection and preparation of patients, may guarantee very low perioperative mortality (approximately 1.0%) after OR of AAA [4].
The long-term results of the EVAR trial 1 are of particular significance regarding the treatment of degenerative AAA in younger, good risk patients [1]. According to this trial, endovascular repair of AAA had a significantly higher total mortality after eight years of follow-up (p=0.048). The increased aneurysm-related mortality in the EVAR group was caused mainly by secondary aneurysm sac rupture (p=0.0064). The incidence of life-threatening reinterventions was also significantly higher in the EVAR group after eight years (p=0.0002) [1]. The previously mentioned meta-analysis showed that in the long term (>8 years) the hazard of aneurysm-related mortality was significantly higher after EVAR (HR 5.12, 95% CI: 1.59-16.44). At the same time, the risk of secondary intervention (HR 2.13, 95% CI: 1.69-2.68), aneurysm rupture (OR 5.08, 95% CI: 1.11-23.31), and death due to rupture (OR 3.57, 95% CI: 1.87-6.80) were also significantly higher after EVAR [3].
After all, it is not unexpected that both the guidelines on the diagnosis and treatment of aortic diseases published by the European Society of Cardiology [5] and the guidelines on the management of AAA published by the European Society for Vascular Surgery (ESVS) [6] recommend that OR should be considered as the preferred treatment modality in patients with long life expectancy. On the other hand, patients with a shorter life expectancy are likely to benefit from EVAR rather than OR, particularly if their surgical risk is higher than average [3,5,6].
Unfavourable aneurysmal anatomy
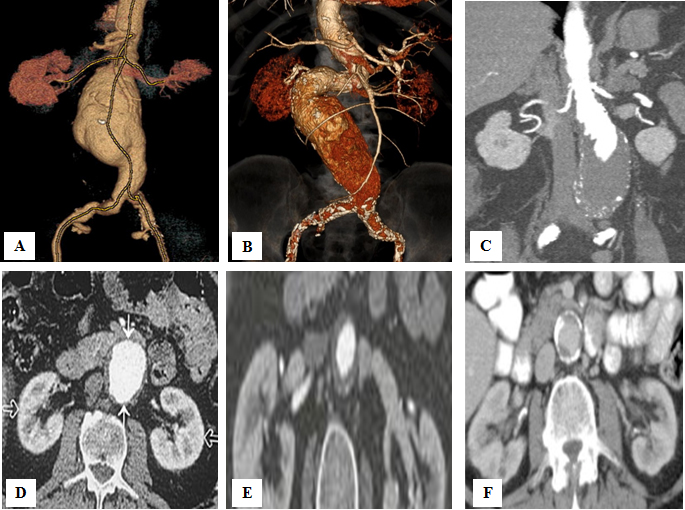
The aneurysmal anatomy is the first factor that can make standard EVAR more difficult or even impossible. According to an FDA study that examined the eligibility of infrarenal AAA for on-label EVAR, 35% of male and up to 60% of female patients were unsuitable for standard EVAR because of problems with aneurysmal neck or iliac access [7]. Severe tortuosity and small diameter of iliac arteries (<6 mm) are the first anatomic limitations for EVAR. However, the characteristics of the aneurysmal neck play a much more important role. A Delphi Consensus document that defines five aneurysm neck hostility criteria (aortic neck diameter, aortic neck angulation, conical neck, aortic neck length, circumferential calcification) was created by nine Italian vascular surgeons from high-volume centres (>50 EVAR procedures/year) in 2019 [8]. This document identified the following categories of patients: those in whom standard EVAR is feasible; those in whom standard EVAR is not the first choice due to anatomic conditions; those in whom standard EVAR is not advised due to moderate risk of failure; those in whom standard EVAR is not advised due to high risk of failure; finally, those in whom standard EVAR is not applicable. According to these criteria, a standard EVAR is not applicable when aneurysmal neck has the following characteristics: length <10 mm, width >32 mm, angulation >750, circumferential calcification of at least 50%, as well as conical shape [8] (Figure 1).
The treatment options for AAAs with hostile neck or juxtarenal AAAs (JAAAs) include fenestrated EVAR (F-EVAR), chimney EVAR (Ch-EVAR) and OR. Seven years ago, Katsargyris et al did not find a significant difference regarding the 30-day mortality between OR (3.4%), F-EVAR (2.4%) and Ch-EVAR (5.3%) in patients with JAAAs. They found that OR is a safe and effective treatment option for good risk patients with JAAAs [9]. Also, the most recently published multicentre study suggests that, in fit patients, open JAAA repair can be performed with acceptable operative risk with durable results in terms of both graft integrity and preservation of renal function [10].
Finally, the ESVS guidelines summarise and recommend that the choice between open and complex endovascular repair of JAAAs depends on the patient`s status and aneurysmal anatomy, as well as on surgical experience and patient preference [6].
Inflammatory AAA
The incidence of inflammatory AAA ranges between 4 and 7% [6,11]. According to the ESVS guidelines, in patients with inflammatory AAA and suitable anatomy, EVAR should be considered a first treatment option [6]. On the other hand, in the current Society for Vascular Surgery practice guidelines on the care of patients with an AAA (American guidelines), there is only the statement that endovascular repair of inflammatory AAA is associated with decreased mortality compared with OR [12]. A systematic review with a total number of 120 inflammatory AAAs from 2009 showed significantly lower total one-year mortality in the EVAR group (OR: 14%; EVAR: 2%, p=0.01), as well as almost the same aneurysm-related one-year mortality (OR: 2%; EVAR: 0%; p=0.3) [11]. Postoperative regression of the hydronephrosis was significantly higher in the open surgical group (OR: 69%; EVAR: 39%; p=0.01). The differences regarding regression of the periaortic inflammation (p=0.3) and 30-day mortality (p=0.1) were not significant [12]. Seventy-six patients with inflammatory and 152 with degenerative AAAs were matched by propensity score analysis, controlling for demographics, baseline comorbidities and AAA parameters (1:2 ratio) in our most recently published retrospective single-centre cohort study [12]. In all patients, an OR was performed. Perioperative mortality was significantly higher in the group with inflammatory AAAs (inflammatory: 5.26%; degenerative: 0.0%; p=0.012). At the same time, patients with inflammatory AAAs had longer in-hospital (p=0.035) and ICU stay (p=0.048), as well as more common intraoperative lesions of adjacent structures (p=0.04). During the follow-up period of at least five years, there was no difference in survival (²=0.07, DF=1, p=0.80) or overall aorta-related complications (²=1.25, DF=1, p=0.26); however, aortic graft infection was more frequent in the inflammatory group (p=0.04) [13].
For all of the previous reasons, EVAR should be considered a first treatment option in the majority of patients with inflammatory AAAs. On the other hand, OR may be preferred if patients with inflammatory AAAs have associated hydronephrosis and are deemed low risk.
Rare forms and special considerations regarding aaa
Mycotic AAA
Mycotic AAAs are uncommon and account for only 0.6% to 2% of all AAAs [6,12,14]. According to the Swedish registry, there is no difference in long-term survival, infection-related complications, or reoperation between in situ open and endovascular repair in patients with mycotic AAA [13]. However, according to my clinic’s experience, surgical excision of mycotic AAA associated with an extra-anatomic axillo-femoral-femoral bypass procedure significantly reduces early mortality and the long-term re-infection rate in comparison to in situ OR [4]. For this reason, it is not easy to accept a recommendation from the current ESVS guidelines dedicated to mycotic AAA [6]. Namely, as per those guidelines, a treatment of mycotic AAA should be considered based on patient status, local routine, and team experience, with endovascular repair being an acceptable alternative to OR. I believe that endovascular repair of mycotic AAA should be considered only in emergency situations as a bridging procedure to open surgery, which is still the gold standard for definitive treatment of mycotic AAA.
Thrombosed AAA
Although mural thrombosis frequently accompanies aneurysmal disease, unlike peripheral aneurysms, complete thrombosis of an AAA is distinctly unusual, with a frequency ranging from 0.7% to 2.8% of those which are surgically managed [15,16]. Literature reports of acute AAA thrombosis are also rare, with fewer than 60 cases published to date [17]. The reasons why both chronic and acute complete AAA thrombosis are rare include large aneurysmal diameter, high intraluminal arterial pressure and high arterial flow. However, both in cases of chronic and in cases of acute complete thrombosis of AAA, EVAR is not feasible.
Associated horseshoe kidney
The co-existence of AAA and horseshoe kidney is rare, occurring in less than 0.2% of patients undergoing aneurysm repair [18,19]. However, horseshoe kidney and some other renal anomalies make it more complex and difficult to repair AAA by either OR and EVAR. First of all, horseshoe kidney can limit access to the distal abdominal aorta during open surgery. On the other hand, the transection of the renal isthmus can result in renal necrosis, haemorrhage, urinary leakage with or without fistula formation, sepsis and postoperative renal insufficiency [18,19]. Besides all the other advantages, EVAR in patients with associated horseshoe kidney enables the preservation of the renal isthmus [20]. However, in patients with associated horseshoe kidney and other renal anomalies, EVAR very often requires a covering of accessory renal arteries to achieve an adequate proximal landing zone [20]. It is always followed by partial renal infarction, which is not recommended in patients with pre-existing renal failure. Both the ESVS guidelines [6] and the American guidelines [12] recommend that accessory renal arteries with a diameter larger than 3 mm should be preserved during either open or endovascular repair of AAA. A preservation of accessory renal arteries is much easier to perform during OR of AAA. Due to this, OR should be considered as the first option if patients with AAA have associated significant accessory renal arteries that would be covered with a stent graft. EVAR is indicated when the covering of these arteries can be avoided.
Hereditable disorders of connective tissues
In comparison to thoracic aneurysms, isolated AAA is a very rare presentation of an hereditable disorder of connective tissues [5]. There are just a few published cases in the literature, including one case treated in our clinic, in a patient with Marfan syndrome [21].
In general, endovascular repair should not be used in either the abdominal or the thoracic aorta in patients with connective tissue disorders. The friability of the aortic wall in patients suffering from connective tissue disease seems to be incompatible with the radial force of stent grafts. At the same time, generalised disease of the entire aorta in patients with hereditable disorders of connective tissues causes additional dilatation in non-treated aortic segments. Therefore, type 1 endoleak and graft migration can occur [22].
For this reason, OR is the method of choice for the treatment of AAA in patients with connective tissue disorders. EVAR might be a life-saving bridge procedure in patients with connective tissue disorders who present with exsanguinations due to aneurysmal rupture. EVAR is also indicated in those patients who are at high risk for OR [6,22].
Late open surgical conversion after EVAR
Besides an improvement in surgical skill as well as new advanced endovascular devices, late open surgical conversion (LOSC) after EVAR is a reality with rates ranging between 0.67% and 22.8% [21]. The most common indications for LOSC after EVAR include different types of endoleak, the enlargement of the aneurysm sac including rupture, as well as stent graft migration and infection [20]. Because of several technical aspects (suprarenal or even supraceliac aortic cross-clamping, a removal of stent graft with active proximal fixation, etc.), LOSC after EVAR is a more complex and risky procedure than primary open AAA repair, with reported perioperative mortality rates among contemporary series ranging up to 22% [23] (Figure 2).
Conclusion
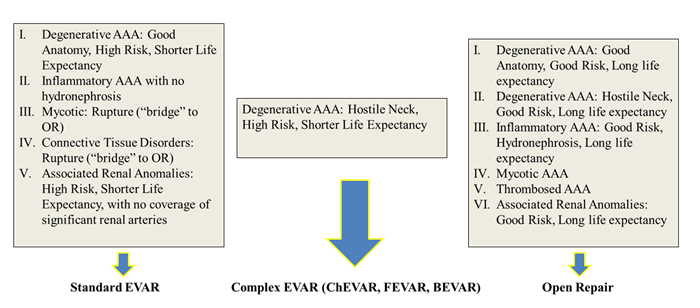
OR should be considered as a first treatment option in patients with degenerative AAA and long life expectancy, while those patients with shorter life expectancy can benefit from EVAR. The choice between open and complex endovascular repair of patients with unfavourable anatomy depends on the patient’s status and aneurysmal anatomy, as well as on surgical experience. EVAR is the first treatment option in the majority of patients with inflammatory AAAs. OR may be preferred in low-risk patients with inflammatory AAAs and associated hydronephrosis. OR is still the gold standard for definitive treatment of mycotic AAA. In cases of complete thrombosis of AAA, EVAR is not feasible. OR should be considered as the first option if patients with AAA have associated significant accessory renal arteries that would be covered with a stent graft. EVAR is indicated when the covering of these arteries can be avoided. OR is the method of choice for the treatment of AAA in patients with connective tissue disorders. EVAR might be a life-saving bridge procedure in those patients who present with aneurysmal rupture, as well as when those patients are at high risk for OR. A referral to a high-volume aortic centre should be considered for repair of AAA. Younger generations of vascular surgeons have to be educated for both endovascular and open repair of AAA.