















Keywords: hypertension definition, treatment goals in different patient categories
Abbreviations
ABPM: ambulatory blood pressure monitoring
ACEI: angiotensin-converting enzyme inhibitor
ARB: angiotensin receptor blocker
BP: blood pressure
CAD: coronary artery disease
CCB: calcium channel blocker
CKD: chronic kidney disease
CV: cardiovascular
CVD: cardiovascular disease
DBP: diastolic blood pressure
EF: ejection fraction
ESC: European Society of Cardiology
ESH: European Society of Hypertension
HBPM: home blood pressure monitoring
HF: heart failure
HMOD: hypertension-mediated organ damage
MI: myocardial infarction
RAS: renin–angiotensin system
RCT: randomised controlled trial
SBP: systolic blood pressure
SCORE: Systemic COronary Risk Evaluation
SPC: single-pill combination
TIA: transient ischaemic attack
Introduction
Hypertension continues to be the most common preventable cardiovascular risk factor for major cardiovascular events in Europe. Blood pressure (BP) control remains largely unsatisfactory. In Europe, >150 million people are affected by hypertension and its prevalence is predicted to rise by 15% to 20% by 2025. Significant efforts have been made in recent decades to improve BP control worldwide [1]. However, the lack of BP control in ≥40% of the population remains a major missed opportunity for European healthcare systems. For this reason, development of new guidelines appeared timely and appropriate.
Therefore, the 2018 ESC/ESH Guidelines on hypertension were developed. The purpose of the review and update of the guidelines was to evaluate and incorporate new evidence into the guideline recommendations. The principal aim was to improve pragmatically the diagnostic accuracy of hypertension and the therapeutic efficacy of antihypertensive management, with the challenging aim of improving BP control and reducing the related cardiovascular burden.
The key novel aspects of the ESC/ESH Guidelines are the improvement of individual cardiovascular risk stratification and BP targets to be achieved, the timing for starting pharmacological treatment and the time to get to target, the prevalent role of initial combination therapy, and the promotion of adherence to treatments [2].
What is new in the 2018 ESC/ESH Arterial Hypertension Guidelines?
1 - Diagnosis (Recommendation; Class I)
It is recommended to base the diagnosis of hypertension on:
- Repeated office BP measurements; or
- Out-of-office BP measurement with ambulatory blood pressure monitoring (ABPM) and/or home blood pressure monitoring (HBPM), if logistically and economically feasible.
2 - Treatment thresholds
a. High normal BP (130–139/85–89 mmHg):
Drug treatment may be considered when cardiovascular (CV) risk is very high due to established cardiovascular disease (CVD), especially coronary artery disease (CAD). (Recommendation; Class IIb)
b. Treatment of low-risk grade 1 hypertension:
In patients with grade 1 hypertension at low/moderate risk and without evidence of hypertension-mediated organ damage (HMOD), BP-lowering drug treatment is recommended if the patient remains hypertensive after a period of lifestyle intervention. (Recommendation; Class I)
c. Older patients:
BP-lowering drug treatment and lifestyle intervention is recommended in fit older patients (>65 years but not >80 years) when systolic blood pressure (SBP) is in the grade 1 range (140–159 mmHg), provided that treatment is well tolerated.(Recommendation; Class I)
3 - BP treatment targets (Recommendation; Class I)
It is recommended that the first objective of treatment should be to lower BP to <140/90 mmHg in all patients and, provided that the treatment is well tolerated, treated BP values should be targeted to 130/80 mmHg or lower in most patients.
In patients <65 years it is recommended that SBP should be lowered to a BP range of 120–129 mmHg in most patients.
In older patients (65–80 years): in older patients (≥65 years), it is recommended that SBP should be targeted to a BP range of 130–139 mmHg.
In patients aged over 80 years: an SBP target range of 130–139 mmHg is recommended, if tolerated.
4 - Diastolic blood pressure (DBP) targets: (Recommendation; Class IIa)
A DBP target of <80 mmHg should be considered for all hypertensive patients, independent of the level of risk and comorbidities.
5 - Initiation of drug treatment: (Recommendation; Class I)
It is recommended to initiate an antihypertensive treatment with a two-drug combination, preferably in a single-pill combination (SPC). The exceptions are frail older patients and those at low risk and with grade 1 hypertension (particularly if SBP is <150 mmHg).
6 - Resistant hypertension: (Recommendation; Class I)
The recommended treatment for resistant hypertension is the addition of low-dose spironolactone to existing treatment, or the addition of further diuretic therapy if intolerant to spironolactone, with either eplerenone, amiloride, higher-dose thiazide/thiazide-like diuretic or a loop diuretic, or the addition of bisoprolol or doxazosin
Definition of hypertension
Hypertension is defined as a persistent elevation in office systolic BP ≥140 and/or diastolic BP ≥90 mmHg, which is equivalent to a 24-hr ABPM average of ≥130/80 mmHg or an HBPM average of ≥135/85 mmHg. This is based on evidence from multiple randomised controlled trials (RCTs) which shows that treatment of patients with these BP values is beneficial. The same classification is used in younger, middle-aged, and older people [3].
Other types and terms of hypertension
1 - White-coat hypertension
White-coat hypertension is defined as an elevated office untreated BP, but is normal when measured by ABPM, HBPM, or both [4]. The difference between the higher office and the lower out-of-office BP is referred to as the “white coat effect”, and is believed to reflect mainly the pressor response to an alerting reaction elicited by office BP measurements by a doctor or a nurse, although other factors are probably also involved [5]. It can account for up to 30 to 40% of people (and >50% in the very old) with an elevated office BP. It is more common with increasing age, in women, and in non-smokers. Its prevalence is lower in patients with HMOD, when office BP is based on repeated measurements, or when a doctor is not involved in the BP measurement. A significant white-coat effect can be seen at all grades of hypertension (including resistant hypertension), but the prevalence of white-coat hypertension is greatest in grade 1 hypertension.
The white-coat effect is used to describe the difference between an elevated office BP (treated or untreated) and a lower home or ambulatory BP in both untreated and treated patients.
2 - Masked hypertension
Masked hypertension refers to untreated patients in whom BP is normal in the office but is elevated when measured by HBPM or ABPM [6]. It can be found in approximately 15% of patients with a normal office BP. The prevalence is greater in younger people, males, smokers, and those with higher levels of physical activity, alcohol consumption, anxiety, and job stress. Obesity, diabetes, chronic kidney disease (CKD), family history of hypertension, and high–normal office BP are also associated with an increased prevalence of masked hypertension. It is associated with dyslipidaemia and dysglycaemia, HMOD [7], adrenergic activation, and increased risk of developing diabetes, and sustained hypertension [6].
3 - Resistant hypertension and pseudo-resistant hypertension
Hypertension is defined as resistant to treatment when the recommended treatment strategy fails to lower office SBP and DBP values to <140 mmHg and/or <90 mmHg, respectively, and the inadequate control of BP is confirmed by ABPM or HBPM in patients whose adherence to therapy has been confirmed. Prevalence studies of resistant hypertension have been limited by variation in the definition used; the reported prevalence rates range from 5–30% in patients with treated hypertension. After applying a strict definition and having excluded causes of pseudo-resistant hypertension, the true prevalence of resistant hypertension is likely to be <10% of treated patients. Patients with resistant hypertension are at higher risk of HMOD, CKD, and premature CV events [8].
Possible causes of pseudo-resistant hypertension are:
- Poor adherence to prescribed medicines
- White-coat phenomenon
- Poor office BP measurement technique
- Marked brachial artery calcification
- Clinician inertia
4 - Secondary hypertension
Secondary hypertension is hypertension due to an identifiable cause, which may be treatable with an intervention specific to the cause. A high index of suspicion and early detection of secondary causes of hypertension are important because interventions may be curative, especially in younger patients; however, interventions later in life are less likely to be curative (i.e., removing the need for antihypertensive medication) because longstanding hypertension results in vascular and other organ damage that sustains the elevated BP. Nevertheless, intervention is still important because it will often result in much better BP control with less medication.
The prevalence of secondary hypertension is reported to be 5–15% [9] of people with hypertension. Screening all hypertensive patients for secondary hypertension is not feasible or cost-effective; it should be confined to some general patient characteristics that suggest those more likely to have secondary hypertension and in whom screening should be considered after confirming that BP is elevated with ABPM.
Terms of hypertension
I - True normotension: is used when both office and out-of-office BP measurements are normal
II - Sustained hypertension: is used when both the above are abnormal.
Terms used for treated hypertensive patients
III - Masked uncontrolled hypertension (MUCH): in which the office BP is controlled but home or ambulatory BP is elevated.
IV - White-coat uncontrolled hypertension (WUCH): the office BP is elevated but home or ambulatory BP is controlled.
V - Sustained uncontrolled hypertension (SUCH): both office and home or ambulatory BP are uncontrolled.
Classification of office blood pressure and definitions of hypertension grade
It is recommended that BP be classified and hypertension graded as follows:
- Optimal - SBP <120 mmHg and DBP <80 mmHg
- Normal - SBP 120-129 mmHg and/or DBP 80-84 mmHg
- High normal - SBP 130-139 mmHg and/or DBP 85-89 mmHg
- Grade 1 - SBP 140-159 mmHg and/or DBP 90-99 mmHg
- Grade 2 - SBP 160-179 mmHg and/or DBP 100-109 mmHg
- Grade 3 - SBP ≥180 mmHg and/or DBP ≥110 mmHg
- Isolated systemic hypertension - SBP ≥140 mmHg and DBP <90 mmHg
Hypertension and total cardiovascular risk assessment
The latest ESC/ESH Guidelines further highlight the importance of the systematic estimation of total cardiovascular risk in individual hypertensive patients, endorsing the paradigm shift from the view of cardiovascular risk factors as separate silos to a more comprehensive assessment of individual total cardiovascular risk profile. Every doctor should systematically estimate individual cardiovascular risk in each hypertensive patient at the time of initial diagnosis or whether any changes occur. In Europe, the Systemic COronary Risk Evaluation (SCORE) system [10] is the most frequently adopted tool for this purpose, and it is now recommended also for individuals aged >65 years.
The importance of HMOD in refining cardiovascular risk assessment in hypertensive patients
Current European guidelines also re-emphasise the importance of detecting HMOD, which may indeed contribute to refining the total cardiovascular risk and the consequent therapeutic strategy [11]. Detection of HMOD should be undertaken for a proper identification of the subjects at higher cardiovascular risk, beyond the SCORE system. This is a way to provide a more realistic assessment of cardiovascular risk and to predict non-fatal cardiovascular events. European guidelines support an approach based on multiplying by threefold the estimated risk of fatal events [2], based on the Framingham algorithm.
Treatment initiation: cut-offs revisited in high or low risk
The degree of hypertension (grades 1–3) determines the initiation of treatment and the individual cardiovascular risk of the patient. Table 1 depicts the grades according to BP levels.
Table 1. Staging of hypertension according to blood pressure levels, and cardiovascular risk factors by the SCORE system. CV risk is illustrated for middle-aged males. The use of the SCORE system is recommended for formal estimation of CV risk for treatment decisions. Reprinted by permission of Oxford University Press on behalf of the European Society of Cardiology from Williams B et al [3].
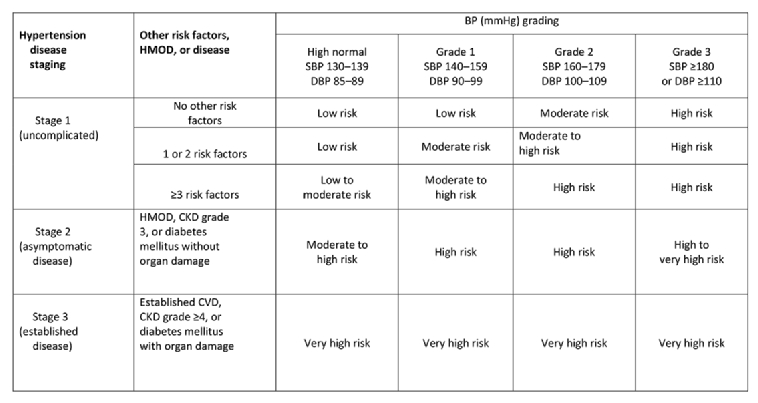
BP: blood pressure; CKD: chronic kidney disease; CV: cardiovascular; DBP: diastolic blood pressure; HMOD: hypertension-mediated organ damage; SBP: systolic blood pressure; SCORE: Systematic COronary Risk Evaluation
Whether pharmaceutical treatment should be initiated immediately or after a delay with lifestyle intervention is focused on high or low cardiovascular risk (Table 1). In lower-risk patients with grade 1 hypertension (defined as office BP 140–159/90–99 mmHg), and without end-organ damage aged up to 80 years old, treatment should be started after a trial of lifestyle changes, e.g., for 3–6 months. On the other hand, for high-risk patients with grade 1 hypertension (140–159/90–99 mmHg), medical drug therapy should be initiated immediately. Patients with grade 2 (160–179/100–109 mmHg) or grade 3 hypertension (≥180/≥110 mmHg) should receive immediate antihypertensive drug treatment along with lifestyle intervention. Lifestyle changes are enforced in the current guidelines, whether before beginning as well as always during ongoing medical treatment.
Target range for blood pressure treatment (Table 2)
The general treatment targets of BP have been lowered to at least 130/80 mmHg for almost all patients. In all patients who can tolerate treatment, the office SBP should be lowered to <140 mmHg. Office diastolic BP should, in general, be lowered to <80 mmHg. In patients younger than 65 years, office systolic BP lower than 130 mmHg should be aimed for, but not below 120 mmHg. In older patients over 65 years, and in old patients up to age 80 years who are capable of an independent lifestyle and are not frail, a target SBP of 130 mmHg but not below 130 mmHg is recommended (Table 2). In old patients >80 years, treatment should generally be initiated in case of an office SBP ≥160 mmHg. In frail patients, individual decisions with gentle reductions are advised according to the benefit expectations of treatment. Importantly, the lower thresholds for BP treatment are now also clearly defined. Systolic BP should not be lowered to below 120 mmHg. Diastolic BP should not be lowered to below 70 mmHg. Therefore, clear target ranges have now been defined with lower BP cut-offs where antihypertensive treatment should not go beyond these values. When starting antihypertensive drugs, the first objective should be to lower BP to <140/90 mmHg in all patients. If the treatment is then well tolerated, BP should be targeted to 130/80 mmHg or lower in most patients; however, treated SBP should not be targeted to <120 mmHg as stated above and DBP not below 70 mmHg.
Table 2. Office blood pressure treatment target range.
Reprinted by permission of Oxford University Press on behalf of the European Society of Cardiology from Williams B et al [3].
/Guidelines/Clinical-Practice-Guidelines/Arterial-Hypertension-Management-of
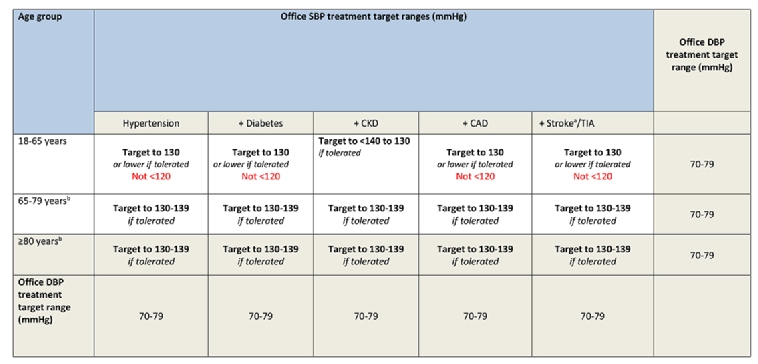
a Refers to patients with previous stroke and does not refer to blood pressure targets immediately after acute stroke.
b Treatment decisions and blood pressure targets may need to be modified in older patients who are frail and independent.
CAD: coronary artery disease; CKD: chronic kidney disease (includes diabetic and non-diabetic CKD); DBP: diastolic blood pressure; SBP: systolic blood pressure; TIA: transient ischaemic attack
Blood pressure targets in specific subgroups of hypertensive patients
Treatment thresholds for office BP are defined as ≥140/≥90 mmHg and are the same in hypertensive patients who also have diabetes, CAD, CKD, stroke or TIA; however, in very high-risk patients with CAD, previous stroke or TIA, treatment may already be considered in high–normal SBP of 130–<140 mmHg. In patients older than 80 years, a threshold of ≥160/≥90 mmHg is advised for all groups, including those with diabetes, CAD, CKD or stroke [12].
Diabetes
For patients with diabetes, the same treatment targets are recommended for an office SBP target of 130 mmHg or lower [13]. SBP should not be lowered to <120 mmHg. The DBP target should be <80 mmHg. In older patients (≥65 years) the SBP target range is 130–140 mmHg if tolerated. A variable visit-to-visit BP should be noted due to associated increased cardiovascular and renal risk. Caution is emphasised in autonomic polyneuropathy concerning postural or orthostatic hypotension. Nocturnal BP should be assessed by 24-hr ABPM in order to detect hypertension in apparently normotensive diabetic patients.
Coronary disease
In CAD, diastolic BP should not be lowered to <70 mmHg as myocardial perfusion may be impaired in lower values [14]. In CAD, treatment is already recommended at the threshold of high–normal BP of 130–139/85–89 mmHg, as these patients are considered to be at very high risk.
Chronic kidney disease
The renin–angiotensin system (RAS) blockers (angiotensin-converting enzyme inhibitor [ACEI] or angiotensin receptor blocker [ARB]) are endorsed as more effective in reducing albuminuria than other antihypertensive drugs. The guidelines recommend an RAS blocker and calcium channel blocker (CCB) as the initial regimen drugs. In either diabetic or non-diabetic CKD, the SBP target is 130–139 mmHg. Individualised treatment is advocated according to electrolytes.
Heart failure
In hypertensive patients with preserved or reduced ejection fraction (EF), antihypertensive treatment should be considered if BP is ≥140/≥90 mmHg. If antihypertensive treatment is not needed, the treatment of heart failure (HF) should follow the current ESC HF Guidelines [15]. In HF with reduced EF, the initial antihypertensive regimen advocates an ACEI or ARB (or angiotensin receptor/neprilysin inhibitor as indicated by guidelines) plus a thiazide diuretic (or loop diuretic in oedema), plus a beta-blocker. The second step adds the mineralocorticoid receptor antagonist spironolactone or eplerenone. Although in general actively lowering the BP below 120/70 mmHg should be avoided, patients may achieve lower values due to HF guideline-directed medications which, if tolerated, should be continued.
Conclusion
The new ESC Guidelines have clearly defined therapeutic targets with lower thresholds, below which treatment should not be continued. In most patients, a BP goal of at least 130/80 mmHg is recommended, but not below 120/70 mmHg. Lifestyle interventions are re-enforced in all stages of hypertension. In particular, the guidelines clearly aim at lowering the high-risk profiles of patients with concomitant cardiovascular diseases, e.g., coronary disease or diabetes.