

















Keywords: bladder, blood pressure, cuff, device, measurement, obesity, oscillometric
Introduction
The characteristics of the optimal cuff for traditional blood pressure (BP) measurement with the mercury sphygmomanometer have been the subject of much debate since the beginning of the 20th century. Even today, there is no general consensus about the appropriate size of cuffs and bladders in relation to the arm circumference [1,2]. That miscuffing may lead to inaccurate BP measurements is a well-known fact. In particular, the use of cuffs and bladders which are too narrow or too short (undercuffing) may lead to overestimation of BP, a problem overlooked by many doctors when measuring BP in the obese [1,2].
The recommendations of leading international scientific societies have often been inconsistent. The American Heart Association (AHA) recommends the use of four different cuffs according to the arm circumference whose sizes are mainly based on the 40% (width) x 80% (length) rule [3]. For upper arm circumferences 22-26 cm, a small adult cuff with a bladder measuring 10 x 24 cm is recommended by the AHA. For arm circumferences ranging from 27 to 34 cm, an adult cuff with a bladder measuring 13 x 30 cm should be used. A large adult cuff with a bladder measuring 16 x 38 cm for arm circumferences 35-44 cm, and an adult thigh cuff with a bladder measuring 20 x 42 cm for arm circumferences 45-52 cm are recommended for obese subjects. At variance with the recommendations of the AHA, the British Hypertension Society recommends for all types of arm a bladder with the same width (12 cm). Only the length of cuff and bladder varies according to the arm size [4].
These inconsistencies are the result of the lack of a gold standard for BP measurement because of the difficulty of obtaining comparative data from intraarterial studies. A noticeable contribution to this issue has been provided by an intraarterial study in which multiple simultaneous indirect BP measurements were made with the cuff width:arm circumference ratio (CWACR) varying from 30 to 55%. This study showed that the optimum cuff width for the indirect measurement of BP is proportional to the logarithm of the arm’s circumference [5]. The optimum CWACR in the 50 subjects investigated in this study was 46.4%, well above the 40% CWACR proposed by the AHA guidelines. However, the problem is even more complex because the optimum CWACR differed in lean and obese subjects. For the subjects with small arms, the optimum CWACR was 49.9%, whereas for the subjects with large arms it was 42.3%.
The advent of oscillometric BP measurement
The above recommendations for traditional auscultatory BP measurement do not necessarily apply to BP measured using the oscillometric method. With the sphygmomanometric technique the role of the cuff is only to compress the artery under a defined reference pressure, whereas with the oscillometric method the cuff is at the same time the signal sensor [2,6] and the reference point is not the artery occlusion but the oscillometric peak signal [6].
In an elegant experiment performed on an arm model, Lan et al showed that the measured cuff pressure oscillations are a reflection of the entire artery volume change under the cuff, thereby presenting a mixture of arterial distension in different closure states during the entire measurement process [7]. In addition, depending on the device algorithm, with oscillometric devices the signal sensing may take place not only at the pressure deflationary phase, but also, or even exclusively, at the inflationary phase. Thus, different criteria may apply to cuffs and bladders used for the oscillometric BP measurement compared to the traditional one. However, little is known about the relationship between cuff size and upper arm circumference for oscillometric monitors which can provide accurate BP readings with the use of cuffs much smaller than those currently recommended (see below). This highlights the importance of different software-cuff combinations when using different measurement methods.
One advantage of the oscillometric over the auscultatory measurement is that stiffness of the brachial artery does not affect the accuracy of oscillometric BP measurement [7]. Brachial artery elasticity affects the pressure transmission from the bladder to the arm surface by about 5% and therefore the auscultatory BP measurement can be overestimated or underestimated by about 5% [7]. With oscillometry, although the oscillation amplitude is smaller with stiff than with elastic arteries, the cuff pressure at which the maximum amplitude oscillations occur is approximately unchanged. This is due to the fact that the oscillometric BP measurement is based on the location and not on the amplitude of the oscillations [6]. As maximum oscillations occur at the same point with any type of arterial wall, the difference in brachial artery stiffness does not affect the accuracy of the oscillometric BP measurements.
Problems with BP measurement in the obese
As mentioned above, obese subjects often require the use of large-sized cuffs. According to the AHA recommendations, for arm circumferences >34 cm a bladder measuring 16 cm in width should be used up to a circumference of 44 cm and a bladder of 20 cm for circumferences from 45 to 52 cm [3]. However, upper arms shorter than 20 cm can be found in at least 20% of individuals [8,9], most often among obese women and, in these subjects, an extra-large arm cannot be correctly cuffed. For these people, the AHA recommends a 16 cm wide bladder [3], but obviously this increases the likelihood of inaccurate BP measurement.
Another problem often overlooked by scientific authorities is the shape of the arm in the obese. Recent evidence has shown that the choice of the appropriate cuff in obese individuals depends not only on the arm circumference but also on its shape [9]. Obese individuals often have a conically shaped arm which makes it difficult to fit a rectangular (cylindrical when worn) cuff to the arm [10]. The tronco-conical shape of the upper arm linearly increases with increasing circumference of the arm (Figure 1). This problem has been totally disregarded in the current guidelines.
Figure 1. Upper arm shape in 569 subjects divided into 4 groups according to upper arm size. Upper α represents the mean slant angle for the truncated cone in each group. Data from Palatini et al (unpublished results).
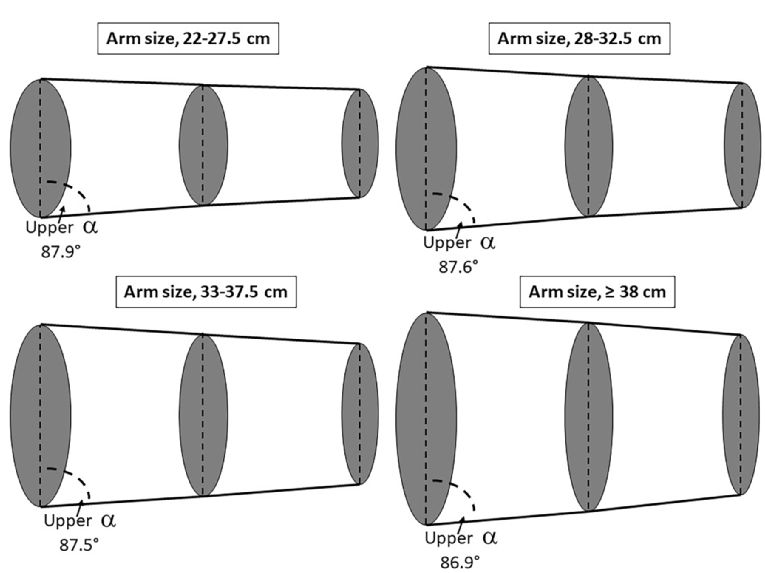
According to data from our laboratory (N=569), the truncated cone slant angle of the upper arm ranges from 89.2° to 82.4° (upper α in Figure 1). In Figure 1 the slant angles for four different groups with increasing upper arm circumference are shown. The mean slant angle linearly increases with increasing arm size. Quite understandably, if a large-size cylindrical cuff is used in conical arms, at the elbow end of the cuff a large gap will remain between the cuff and the arm surface which will cause an irregular expansion of the cuff over the distal part of the arm. In subjects with large arms this may cause an overestimation of BP with systolic BP differences as large as 10 mmHg [9], even when cuffs of an appropriate size are used. This measurement error is particularly pronounced in subjects with morbid obesity and arm circumference of 42 cm or larger in whom the cylindrical cuff overestimated BP on average by 5/3 mmHg [11].
The wide-range cuff
To overcome the problem of miscuffing in obese people with a short humerus length, special cuffs that can accommodate a wide range of arm sizes from medium to very large have been developed [2,12,13]. These so-called “wide-range” cuffs contain smaller bladders than those currently recommended by scientific bodies, yet they proved to yield accurate BP measurements over a wide range of arm circumferences thanks to a special software algorithm. The correct reference pressure in the cuff is reached through a specific cuff design which can provide stable arterial occlusion and assessment of the oscillometric signal efficiency in the software algorithm through electronic gain adjustment in each measurement.
In our laboratory, in a group of subjects with arm circumferences ranging from 32 cm to 50 cm, we demonstrated that an oscillometric device could provide accurate BP readings when coupled to a cuff with a 14.5 x 32 cm bladder, well below the size recommended by the AHA or other scientific societies [14]. However, adoption of a tronco-conical shape may also be crucial for wide-range cuffs. Indeed, it has been shown that, when a cylindrical wide-range cuff was used in obese subjects, it consistently overestimated systolic BP [12]. In contrast, when a tronco-conical cuff was used, accurate BP readings were obtained.
Other BP measurement options in the obese
In obese individuals with a short upper arm, a valid alternative may be the use of devices that measure BP at the forearm. Recently, manufacturers have produced conically shaped cuffs for forearm monitors intended for obese patients. One such device has been validated against the intraarterial measurement in 34 subjects whose forearm upper circumference was 30 cm and distal circumference was 18 cm, denoting a clear tronco-conical shape [15]. Using a tronco-conical cuff, this device provided reliable BP readings; the measurement error was totally unrelated to the forearm circumference, being fairly constant across the whole range of forearm sizes [15]. In obese subjects in general, and especially in subjects with short upper arm, the use of wrist monitors may also be considered. In the last few years, many validated wrist devices have appeared on the market with the advantage of being smaller and easier to fit than upper-arm monitors, thus being suitable for BP measurement in the obese. However, in spite of technical improvement, their reliability in real-life conditions is still controversial because the accuracy of BP measurement at the wrist largely depends on the difference in height between the wrist and the heart.
In a recent study, we showed that the relationship between BP measured at the upper arm and at the wrist varied according to whether BP measurements were made in the office under a doctor’s supervision or at home in a real-life situation [16]. When BP was taken in the office, the values measured at the wrist were close to those measured at the upper arm. In contrast, when BP was self-measured at home by the study participants, higher BP values were obtained at the wrist than at the arm [16]. Thus, it appears prudent to discourage the use of wrist devices, at least in persons with cognitive deterioration.
Conclusions
In obese individuals, the use of a cuff with an optimal size and shape in relation to the patient’s arm is of primary importance. The shape of the cuff is crucial for obtaining reliable BP readings, and in subjects with large arms it should always be tronco-conical [17]. However, information on the appropriate slant angle that should be adopted for cuffs and bladders in relation to arm sizes is scanty. The results obtained with oscillometric devices that make use of wide-range cuffs look promising and may represent the best option for BP measurement in the very obese. However, the good performance of these cuffs should be confirmed in larger samples.