Introduction
Aortic stenosis (AS) is the most frequent valvular heart disease in patients referred to hospital, accounting for 40 to 50% of patients with a diagnosis of valvular disease [1,2]. The incidence of AS increases sharply after the age of 65, explaining why its prevalence reaches 5% after the age of 80 [3]. Moreover, the number of patients with AS is expected to be multiplied by 2 to 3 in the next 50 years [4]. AS is therefore a disease encountered frequently by the general cardiologist. In the 2017 issue of the European Society of Cardiology (ESC)/European Association of Cardio-Thoracic Surgery (EACTS) Guidelines on valvular heart disease, the section dedicated to AS has been the subject of a number of updates with regard to the evaluation of and indications for interventions [5]. We will review here the main changes concerning the assessment of the severity of AS and indications for surgery. Indications for transcatheter aortic valve implantation (TAVI) are detailed in a separate paper.
Assessment of the patient with as
Assessment of AS severity
Even if this is not new, guidelines continue to highlight the importance of auscultation for the detection of a murmur, which remains the only means to detect AS in asymptomatic patients and to draw attention to valvular disease in symptomatic patients. In a recent survey on European patients aged 65 or older, only 24% of respondents stated that their general practitioner used a stethoscope at every visit and 16% said that they never used a stethoscope [6].
Figure 1. Stepwise integrated approach for the assessment of aortic stenosis severity (Reproduced with permission of Oxford University Press on behalf of the European Society of Cardiology. © The European Society of Cardiology 2017. All rights reserved). [5]
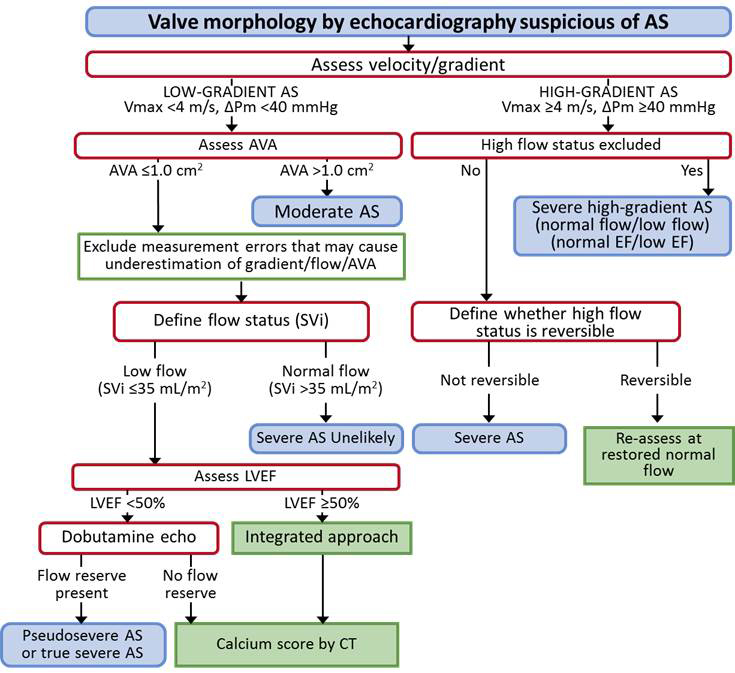
High flow may be reversible in settings such as anaemia, hyperthyroidism, arteriovenous shunts.
Pseudosevere AS is defined by an increase to an AVA >1.0 cm2 with flow normalisation.
ΔPm: mean transvalvular pressure gradient; AS: aortic stenosis; AVA: aortic valve area; CT: computed tomography; EF: ejection fraction; LVEF: left ventricular ejection fraction; SVi: stroke volume index; Vmax: peak transvalvular velocity
Once the diagnosis is confirmed by echocardiography, the first question is the assessment of the severity of AS, which is summarised in Figure 1. In previous ESC/EACTS guidelines, severe AS was defined according to an integrative approach combining aortic valve area, peak aortic jet velocity and mean aortic gradient [7]. In the 2017 ESC guidelines, the first step considers only flow-dependent indices, i.e., peak velocity ≥4 m/sec or mean gradient ≥40 mmHg to reach a conclusion of severe AS regardless of valve area, provided there is no high flow status, e.g., anaemia, hyperthyroidism, liver cirrhosis, arteriovenous shunts. Aortic valve area is taken into account only when peak velocity is <4 m/sec and mean gradient <40 mmHg. AS is moderate if valve area is >1.0 cm2, whereas the diagnosis of low-flow, low-gradient severe AS is likely if valve area is ≤1.0 cm2, provided errors of measurements have been carefully excluded. It is mandatory, in particular, to rule out an underestimation of flow-dependent indices when the Doppler beam is not aligned with the aortic flow. The use of a continuous-wave Doppler probe with multiple echocardiographic windows is particularly important in this setting and may lead to reclassifying 21% of patients [8]. In addition, low-flow, low-gradient severe AS should be confirmed by an indexed stroke volume <35 ml/m2. If left ventricular ejection fraction (LVEF) is <50%, dobutamine stress echo is indicated. If LVEF is ≥50%, the diagnosis of paradoxical low-flow, low-gradient severe AS requires an integrated approach, taking into account clinical criteria and other imaging criteria derived from echocardiography and calcium score as assessed by multislice computed tomography (Table 1) [5].
Table 1. Criteria that increase the likelihood of severe aortic stenosis in patients with aortic valve area <1.0 cm2 and mean gradient <40 mmHg in the presence of preserved ejection fraction. ESC/EACTS Guidelines on valvular heart disease [5].
- Clinical criteria
- Typical symptoms without other explanation
- Elderly patient (>70 years)
- Qualitative imaging data
- Left ventricular hypertrophy (additional history of hypertension to be considered)
- Reduced left ventricular longitudinal function without other explanation
- Quantitative imaging data
- Mean gradient 30−40 mmHga
- Aortic valve area ≤0.8 cm2
- Low flow (SVi <35 mL/m2) confirmed by techniques other than standard Doppler technique (left ventricular outflow tract measurement by 3D TOE or MSCT; CMR, invasive data)
- Calcium score by MSCTb
- Severe aortic stenosis very likely: men ≥3,000; women ≥1,600
- Severe aortic stenosis likely: men ≥2,000; women ≥1,200
- Severe aortic stenosis unlikely: men <1,600; women <800
a Haemodynamics measured when the patient is normotensive.
b Values are given in arbitrary units using Agatston method for quantification of valve calcification.
3D: three-dimensional; CMR: cardiovascular magnetic resonance imaging; MSCT: multislice computed tomography; SVi: stroke volume index; TOE: transoesophageal echocardiography
These changes in the assessment of AS severity are of importance in clinical practice to avoid both underestimation of AS severity and excess diagnosis of low-flow, low-gradient AS. As compared with the estimation of valve area using a continuity equation, flow-dependent indices have the advantage of being associated with a lower likelihood of errors of measurement and possibly underestimating, but not overestimating AS severity. A more detailed approach of issues related to AS severity assessment can be found in a position paper from the European Association of Cardiovascular Imaging [9].
Additional diagnostic and prognostic assessments
Exercise testing remains indicated in patients with severe AS who claim to be asymptomatic since it reveals objective dyspnoea in approximately one third of the patients, which is associated with a high likelihood of developing symptoms in the short term. The additional prognostic value of findings observed during exercise echocardiography has been challenged in recent studies and their usefulness has been downgraded in the 2017 ESC/EACTS Guidelines on valvular disease.
Computed tomography (CT) of the ascending aorta should be performed when aortic enlargement is suspected or proven according to echocardiography to ensure an optimal visualisation of the entire thoracic aorta. This is of particular importance in patients with a bicuspid aortic valve in whom an aneurysm of the ascending aorta is associated in approximately half of the cases. CT of the complete aortic tree and its proximal branches is indicated when TAVI is considered.
Coronary angiography remains indicated in most patients with AS to detect coronary artery disease before an intervention on the aortic valve. The use of computed tomography, as an alternative to coronary angiography, is now a class IIa recommendation in the 2017 ESC/EACTS Guidelines, but only in patients who have a low likelihood of coronary disease, which is rare in patients with AS due to the predominance of AS in the elderly. Except in very rare cases where echocardiography is not conclusive, coronary angiography should not be combined with retrograde left ventricular catheterisation to assess AS severity.
Natriuretic serum peptide levels should be assessed in asymptomatic patients with severe AS.
Indications for surgical aortic valve replacement
Asymptomatic patients
With the wide use of echocardiography, AS is now often diagnosed in patients who do not complain of any symptoms. Asymptomatic AS is thus frequently encountered in general cardiology practice.
Unlike symptomatic patients, asymptomatic patients have a very low risk of complications of AS, in particular of sudden death. At the present time, there is no evidence that the risk of complications outweighs the risk of valvular intervention and that is the reason why intervention is not indicated in all asymptomatic patients with severe AS. Therefore, surgery should theoretically be considered only when symptoms occur. However, there are limitations to this attitude in clinical practice since symptoms are highly variable from one patient to another. More importantly, symptoms are often progressive and may be underreported, thereby exposing patients to a significant amount of time with symptoms before surgery. This is attested to by a prospective series including 103 patients aged 70 or older followed for asymptomatic severe AS [10]. Three-year event-free survival was only 30%, mostly due to indications for aortic valve replacement. More importantly, although patients were prospectively followed in a heart valve clinic every six months, 31% of patients, and 43% of those who developed symptoms, presented with severe symptoms, thereby increasing the risk of intervention. This illustrates the difficulty of symptom interpretation and the potential drawbacks of a watchful waiting attitude. Asymptomatic patients with severe AS should therefore be carefully evaluated to identify those who are at high risk of presenting cardiac events in the short term and who may benefit from early surgery, in particular if it is at low risk.
Observational series have identified factors associated with a high risk of early symptom occurrence and form the basis of the strategy recommended for evaluating asymptomatic patients with severe AS according to the 2017 ESC/EACTS Guidelines on valvular disease (Figure 2).
Figure 2. Management of severe aortic stenosis (Reproduced with permission of Oxford University Press on behalf of the European Society of Cardiology. © The European Society of Cardiology 2017. All rights reserved). [5]
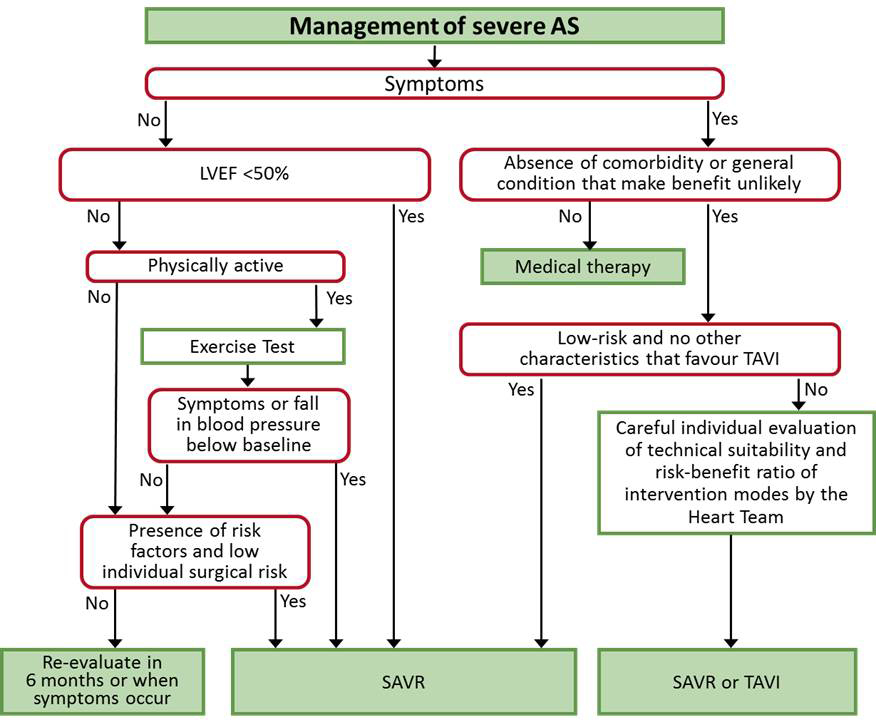
See Figure 1 and Table 1 for the definition of severe AS.
Surgery should be considered (IIa C) if one of the following is present: peak velocity >5.5 m/s; severe valve calcification; peak velocity progression ≥0.3 m/s per year; markedly elevated neurohormones (>threefold age- and sex-corrected normal range) without other explanation; severe pulmonary hypertension (systolic pulmonary artery pressure >60 mmHg).
AS: aortic stenosis; LVEF: left ventricular ejection fraction; SAVR: surgical aortic valve replacement; TAVI: transcatheter aortic valve implantation
- The first step is to assess LVEF. If LVEF is ≤50% without any cause other than AS, there is a class I indication for surgery. Impaired LVEF is, however, infrequent in asymptomatic severe AS.
- When LVEF is >50% and the patient physically active, exercise testing is recommended to unmask symptoms and to search for inadequate rise in blood pressure. Symptoms occurring during exercise testing are a class I indication for surgery. A fall in blood pressure at exercise as compared to baseline is a class IIa indication for surgery.
- When exercise testing is negative or not feasible, other risk factors should be searched and should lead to surgery being considered if it is at low risk (Table 2). These are peak aortic jet velocity and its evolution over time, serum B-type natriuretic peptide (BNP) levels and pulmonary artery pressure.
Table 2.Recommendations for surgical aortic valve replacement in asymptomatic patients with severe aortic stenosis. ESC/EACTS Guidelines on valvular heart disease [5].
- SAVR is indicated in asymptomatic patients with severe aortic stenosis and systolic left ventricular dysfunction (LVEF <50%) not due to another cause.
- Classa: I
- Levelb: C
- SAVR is indicated in asymptomatic patients with severe aortic stenosis and abnormal exercise test showing symptoms on exercise clearly related to aortic stenosis.
- Classa: I
- Levelb: C
- SAVR should be considered in asymptomatic patients with severe aortic stenosis and abnormal exercise test showing fall in blood pressure below baseline.
- Classa: IIa
- Levelb: C
- SAVR should be considered in asymptomatic patients with normal ejection fraction and none of the above-mentioned exercise test abnormalities if the surgical risk is low and one of the following findings is present:
- Very severe aortic stenosis defined by a peak transvalvular velocity >5.5 m/s
- Severe valve calcification and a rate of peak transvalvular velocity progression ≥0.3 m/s per year
- Markedly elevated BNP levels (>threefold age and sex-corrected normal range) confirmed by repeated measurements without other explanations
- Severe pulmonary hypertension (systolic pulmonary artery pressure at rest >60 mmHg confirmed by invasive measurement) without other explanation
- Classa: IIa
- Levelb: C
a Class of recommendation.
b Level of evidence.
BNP: B-type natriuretic peptide; LVEF: left ventricular ejection fraction; SAVR: surgical aortic valve replacement
As compared with the 2012 ESC/EACTS Guidelines on valvular disease, changes in recommendations for surgery in asymptomatic severe AS are the following:
- Severe pulmonary hypertension (systolic pulmonary artery pressure at rest >60 mmHg confirmed by invasive measurement) without other explanation is now a class IIa recommendation for intervention.
- Elevated BNP levels have been upgraded from IIb to a IIa recommendation.
- The increase of mean pressure gradient >20 mmHg during exercise echocardiography was a IIb recommendation and is no longer a recommendation in 2017.
- Excessive left ventricular hypertrophy in the absence of hypertension was a IIb recommendation and is no longer a recommendation in 2017.
It should be acknowledged that all recommendations for surgery in patients with asymptomatic severe AS are based on low levels of evidence, as indicated by C levels of evidence for all of them. Indications are based on the identification of factors associated with a high rate of events during short-term follow-up, but most events are aortic valve replacement due to symptom occurrence. The only studies supporting a benefit of aortic valve replacement on the survival of asymptomatic patients with severe AS are non-randomised observational series with potential source of bias inherent to study design, in particular residual confounding [11,12].
Current recommendations consider only surgical aortic valve replacement in asymptomatic patients. Since TAVI is considered only in patients at increased risk for surgery, risk-benefit analysis does not presently support indications for TAVI in asymptomatic patients.
Hopefully, higher levels of evidence will be available in the near future with the results of two ongoing randomised controlled trials, the AVATAR trial testing surgical aortic valve replacement and the EARLY TAVR trial testing TAVR, both trials including only asymptomatic patients with severe AS.
Symptomatic patients
Symptom occurrence remains the major prognostic factor in the natural history of AS. Intervention is therefore recommended with a class I, level of evidence B, in symptomatic patients with high-gradient severe AS, as defined by a mean gradient ≥40 mmHg or peak velocity ≥4.0 m/s) [5]. The only exception concerns patients with severe comorbidities when the intervention is unlikely to improve quality of life or survival.
In symptomatic patients with low-flow, low-gradient AS, indications for intervention are:
- Class I in the presence of reduced LVEF and evidence of flow (contractile) reserve excluding pseudosevere AS (upgrade from IIa in 2012 Guidelines).
- Class IIa in the presence of reduced LVEF without flow (contractile) reserve, particularly when CT calcium scoring confirms severe AS (upgrade from IIb in 2012 Guidelines).
- Class IIa in the presence of preserved LVEF after careful confirmation of severe AS according to criteria detailed in Table 1.
When an intervention is indicated in symptomatic patients, surgical aortic valve replacement remains the reference treatment in patients at low risk for surgery, as defined by a predicted postoperative mortality <4%. The choice between surgical aortic valve replacement and TAVI in other patients is detailed in a specific article.
Conclusion
The different presentations of AS are covered by the 2017 ESC/EACTS Guidelines which take into account recent improvements in the knowledge of AS. Severity assessment has been simplified for the most frequent presentation of high-gradient AS. Indications for intervention are detailed according to the haemodynamic presentation of AS (low-flow, low-gradient or high-gradient AS) and to the presence of symptoms. The definition of the first-line approaches to be used for severity assessment and risk stratification are important for the practice of general cardiologists, who play a key role in referring the appropriate patients to hospital.