

















Keywords
acute pericarditis, aspirin, colchicine, corticosteroids, management, non-steroidal anti-inflammatory drugs
Introduction
Regarding clinical management and therapy of acute pericarditis, it is not mandatory to search for the aetiology in all patients, especially in countries with a low prevalence of tuberculosis (TB) because of the relatively benign course associated with the common causes of pericarditis and the relatively low yield of diagnostic investigations [1]. The initial evaluation should be focused on screening for specific risk factors that would alter the appropriate treatment [2]. The predictors that have been identified as being associated with an increased risk of complications during follow-up are tamponade, recurrences and constriction. The major risk factors associated with poor prognosis in acute pericarditis include high fever, subacute course, evidence of large pericardial effusion, cardiac tamponade and failure to respond within seven days to non-steroidal anti-inflammatory drugs (NSAIDs). Other predictors, called minor risk factors, should also be considered. These are based on expert opinion and literature review, including acute pericarditis associated with immunodeficiency, trauma, anticoagulant therapy and myocarditis (myopericarditis). On this basis, a triage for acute pericarditis is proposed (Figure 1). Any clinical presentation that may suggest an underlying aetiology (e.g. a systemic inflammatory disease) or with at least one predictor of poor prognosis (major or minor risk factors) warrants hospital admission and an aetiology search. Patients without signs and symptoms of systemic inflammatory disease can be managed as outpatients with empiric anti-inflammatories and short-term follow-up after one week to assess the response to treatment. In patients identified with a cause other than viral infection, specific therapy appropriate to the underlying disorder is indicated, and the epidemiological background (high vs. low prevalence of TB) should be considered [3].
Figure 1. Proposed Triage of Acute Pericarditis.
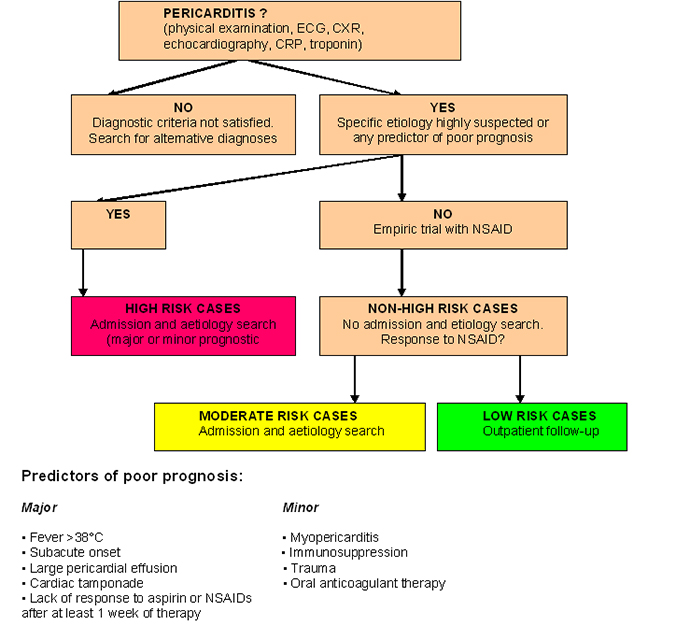
CRP: C-reactive protein; ECG: electrocardiogram
Proposed triage of acute pericarditis according to epidemiological background and predictors of poor prognosis at presentation (at least one predictor of poor prognosis is sufficient to identify a high-risk case). Major criteria have been validated by multivariate analysis, minor criteria are based on expert opinion and literature review. Cases with moderate risk are defined as those without a negative prognostic predictor, but incomplete or lacking response to NSAIDs therapy. Low risk includes those without a negative prognostic predictor and good response to NSAIDs therapy. Specific aetiology is intended as non-idiopathic.
(Adapted with permission from Adler et al. 2015 ESC guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC) Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS), with permission from Oxford University Press. [3])
General recommendations, physical activity and lifestyle changes
The first non-pharmacological recommendation is to restrict physical activity to no more than is usual for patients not involved in competitive sports until symptoms have been resolved and the diagnostic tests normalised (i.e. CRP, ECG and echocardiogram). A minimal restriction of three months (after the initial onset of the attack) is suggested to be applied only to athletes. A shorter period (until remission) may be suitable for non-athletes [4,5].
Prognosis
Most patients with acute pericarditis (generally those with presumed viral or idiopathic pericarditis) have a good long-term prognosis [6]. Cardiac tamponade rarely occurs in patients with acute idiopathic pericarditis, and is more common in patients with a specific underlying aetiology, such as malignancy, TB or purulent pericarditis. The risk of developing constriction can be classified as low (1%) for idiopathic and presumed viral pericarditis, intermediate (2-5%) for autoimmune, immune-mediated and neoplastic aetiologies, and high (20-30%) for bacterial aetiologies, especially with TB and purulent pericarditis. Approximately 15-30% of patients with idiopathic acute pericarditis who are not treated with colchicine will develop either recurrent or incessant disease, while colchicine may halve the recurrence rate. The proposed triage of acute pericarditis according to epidemiological background and predictors of poor prognosis is presented in Figure 1 [3].
Pharmacologic therapy for acute pericarditis
Aspirin or NSAIDs are mainstays of therapy for acute pericarditis [7]. If laboratory data support the clinical diagnosis, symptomatic treatment with NSAIDs should be initiated. Because of its excellent safety, the preferred NSAIDs is ibuprofen in a dose of 600 to 800 mg orally, three times daily with discontinuation if pain is no longer present after two weeks [8]. Many patients have very gratifying responses to the first or second dose of NSAIDs, and most respond fully with no need for additional treatment. The choice of drug should be based on the medical history of the patient, including contraindications, previous efficacy or side effects, the presence of concomitant diseases favouring aspirin over other NSAIDs when aspirin is already needed as an antiplatelet treatment, and finally the physician's expert skills and knowledge [9]. Reliable patients with no more than small effusions, who respond well to NSAIDs, need not be admitted to hospital [10]. Patients who do not respond well initially, who have larger effusions, or who have a suspected cause other than idiopathic pericarditis should be hospitalised for additional observation, diagnostic testing and treatment. Patients who respond slowly or inadequately to NSAIDs may require supplementary narcotic analgesics to allow time for a full response or a course of colchicine [11]. Colchicine is recommended at low, weight-adjusted doses to improve the response to medical therapy and to prevent recurrences [12].
Colchicine is administered as a 2-to-3-mg oral loading dose followed by 1 mg daily for three months [13]. It is unusual not to achieve a satisfactory response to a regimen of NSAIDs with colchicine added. Colchicine has been proposed as a standard adjuvant to NSAIDs for initial treatment [14]. The dosing of the most commonly prescribed anti-inflammatory therapy for acute pericarditis is presented in Table 1 [3].
Table 1. Dosing of the Most Commonly Prescribed Anti-Inflammatory Therapy for Acute Pericarditis.
- Aspirin
- Usual Dosing: 750-1,000 mg every 8 hr.
- Treatment Duration: 1-2 weeks
- Tapering: Decrease doses by 250-500 mg every 1-2 weeks
- Ibuprofen
- Usual Dosing: 600 mg every 8 hr.
- Treatment Duration:1-2 weeks
- Tapering:Decrease doses by 200-400 mg every 1-2 weeks
- Colchicine
- Usual Dosing: 0.5 mg once (<70 kg) or 0.5 mg twice daily (>70 kg)
- Treatment Duration: 3 months
- Tapering:Not mandatory, alternatively 0.5 mg every other day (<70 kg) or 0.5 mg once (>70 kg) in the last weeks
*Tapering should be considered for aspirin and non-steroidal anti-inflammatory drugs.
Therapy duration is symptoms-and-CRP guided, but generally one to two weeks for uncomplicated cases. Gastroprotection should be provided. Colchicine is added on top of aspirin or NSAIDs.
(Adapted with permission from Adler et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC). Endorsed by the European Association for Cardio-Thoracic Surgery (EACTS), with permission from Oxford University Press. [3])
Poorly responding patients have typically been treated with short courses of corticosteroids [15]. Corticosteroids should be considered as a second option in patients with contraindications and failure of aspirin or NSAIDs because of the risk of favouring the chronic evolution of the disease and promoting drug dependence. In this case they are used with colchicine. However, corticosteroids should be avoided as they appear to encourage recurrences [16]. If they simply cannot be avoided to manage an initial episode, it is recommended to use prednisone, low to moderate doses 0.2-0.5 mg/kg/day or equivalent instead of high doses (i.e. prednisone 1.0 mg/kg/day or equivalent). The initial dose should be maintained until resolution of symptoms and normalisation of CRP, then tapering should be considered. Table 2 presents a summary of the ESC recommendations for the treatment of acute pericarditis [3].
Table 2. Recommendations for the Treatment of Acute Pericarditis
- Aspirin or NSAIDs are recommended as first-line therapy for acute pericarditis with gastroprotection.
- Class a: I
- Level b: A
- Ref. c: 17
- Colchicine is recommended as first-line therapy for acute pericarditis as an adjunct to aspirin/NSAID therapy.
- Class a: I
- Level b: A
- Ref. c: 11-13,21
- Serum CRP should be considered to guide the treatment length and assess the response to therapy.
- Class a: IIa
- Level b: C
- Low-dose corticosteroids should be considered for acute pericarditis in cases of contraindication/failure of aspirin/NSAIDs and colchicine, and when an infectious cause has been excluded, or when there is a specific indication such as autoimmune disease.
- Class a: IIa
- Level b: C
- Exercise restriction should be considered for non-athletes with acute pericarditis until resolution of symptoms and normalisation of CRP, ECG and echocardiogram.
- Class a: IIa
- Level b: C
- For athletes, the duration of exercise restriction should be considered until resolution of symptoms and normalisation of CRP, ECG and echocardiogram - at least 3 months is recommended.
- Class a: IIa
- Level b: C
- Corticosteroids are not recommended as first-line therapy for acute pericarditis.
- Class a: III
- Level b: C
CRP: C-reactive protein; ECG: electrocardiogram; NSAIDs: non-steroidal anti-inflammatory drugs
a Class of recommendation. b Level of evidence. c Reference(s) supporting recommendations. d Added to colchicine.
(Adapted with permission from Adler et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC). Endorsed by the European Association for Cardio-Thoracic Surgery (EACTS), with permission from Oxford University Press. [3])
Management of incessant and recurrent pericarditis
The task force suggests that the term 'acute' should be adopted for new-onset pericarditis, 'incessant' for pericarditis with symptoms persisting for four to six weeks, and 'chronic' for pericarditis lasting more than three months [3]. Recurrent pericarditis is diagnosed with a documented first episode of acute pericarditis, a symptom-free interval of four to six weeks or longer and evidence of subsequent recurrence of pericarditis. The recurrence rate after an initial episode of pericarditis ranges from 15 to 30%, and may increase to 50% after a first recurrence in patients not treated with colchicine, particularly if treated with corticosteroids [15].
Aspirin or NSAIDs remain the mainstay of therapy. Colchicine is recommended on top of standard anti-inflammatory therapy, without a loading dose and using weight-adjusted doses [11]. In cases of incomplete response to aspirin/NSAIDs and colchicine, corticosteroids may be used, but they should be added at low-to- moderate doses to aspirin/NSAIDs and colchicine as triple therapy. They should not used to replace these drugs in order to achieve better control of symptoms. Corticosteroids at low-to-moderate doses (i.e. prednisone 0.2-0.5 mg/kg/day) should be avoided if infections, particularly bacterial and TB, cannot be excluded and should be restricted to patients with specific indications (i.e. systemic inflammatory diseases, post-pericardiotomy syndromes, pregnancy) or NSAID contraindications (true allergy, recent peptic ulcer or gastrointestinal bleeding, oral anticoagulant therapy when the bleeding risk is considered high or unacceptable) or intolerance or persistent disease despite appropriate doses [15]. Although corticosteroids provide rapid control of symptoms, they favour chronicity, more recurrences and side effects. If corticosteroids are used, their tapering should be particularly slow. A critical threshold for recurrences is a 10-15 mg/day dose of prednisone or equivalent. At this threshold, very slow decrements as small as 1.0-2.5 mg at intervals of two to six weeks are useful. In cases of recurrence, every effort should be made not to increase the dose or to reinstate corticosteroids [3]. After obtaining a complete response, tapering should be done with a single class of drug at a time before colchicine is gradually discontinued (over several months in the most difficult cases). Actually, for colchicine, at least six months of therapy is recommended [12]. Recurrences are possible after discontinuation of each drug. Each tapering should be attempted only if symptoms are absent and CRP is normal [13]. Prognosis is generally benign. The complication rates are related to the aetiology and not to the number of recurrences. Drug treatment should take into account this favourable outcome to avoid more toxic agents [14]. However, quality of life can be severely affected in patients with repeated recurrences, subacute or incessant pericarditis and glucocorticoid dependence [3].
Management of specific forms of acute pericarditis
Myopericarditis
Pericarditis and myopericarditis share common aetiologies and overlapping forms may be encountered in clinical practice [3]. Pericarditis with known or clinically suspected concomitant myocardial involvement should be referred to as 'myopericarditis', while predominant myocarditis with pericardial involvement should be referred to as 'perimyocarditis', according to task force consensus. Viral infections are among the most common causes for myopericarditis in developed countries. Other infectious causes are most common in developing countries (especially TB). Hospitalisation is recommended for diagnosis and monitoring of patients with myocardial involvement and differential diagnosis, especially with acute coronary syndromes. The management of myopericarditis is similar to that recommended for pericarditis. Empirical anti-inflammatory therapies (i.e. aspirin 1,500-3,000 mg/day) or NSAIDs (ibuprofen 1,200-2,400 mg/day or indomethacin 75-150 mg/day) are usually prescribed to control chest pain, while corticosteroids are prescribed as a second choice in cases of contraindications, intolerance or failure of aspirin/NSAIDs [18]. There is insufficient data to recommend the use of colchicine. Rest and avoidance of physical activity beyond normal sedentary activities are recommended for all patients with myopericarditis [5,6]. Myocardial involvement in pericarditis has a good prognosis and demonstrates no evolution to heart failure or mortality in patients with myopericarditis [19].
Acute viral pericarditis
This disease often presents as self-limiting, with most patients recovering without complications [1]. The therapy includes a short course of treatment with NSAIDs, with colchicine as adjunct, especially for prevention of recurrences [7]. Some experts suggest antiviral treatment similar to that for myocarditis, although this approach is still under evaluation and rarely used [18]. Importantly, corticosteroids are generally not indicated in viral pericarditis, as they are known to reactivate many virus infections and thus lead to ongoing inflammation [15].
Bacterial pericarditis
Bacterial pericarditis is relatively uncommon in clinical practice in developed countries with a low prevalence of TB. Tuberculous pericarditis is the most common form all over the world and the most common cause of pericardial diseases in developing countries [1]. The management of TB pericarditis includes a couple of steps [7]. Tuberculosis not endemic in the population requires systematic investigation and fails to yield a diagnosis of TB pericarditis. In this case, there is no justification for starting anti-TB treatment empirically. In endemic areas, empiric anti-TB chemotherapy is recommended for exudative pericardial effusion after excluding other causes such as malignancy, uraemia, trauma, purulent pericarditis, and autoimmune diseases [11]. Adjunctive steroids may be considered in HIV-negative cases of TB pericarditis and avoided in HIV-associated TB pericarditis. Therapeutic pericardiocentesis is absolutely indicated in the presence of cardiac tamponade. A 'therapeutic'
biopsy should be considered as part of surgical drainage in patients with cardiac tamponade, those relapsing after pericardiocentesis, or those requiring open drainage of pericardial fluid for reasons such as repeated accumulation of pericardial fluid, or failure to respond to empiric medical therapy. The recommendations are for at least three to four days of subsequent catheter drainage [3].
Purulent pericardial effusions
Purulent pericardial effusions are likely to recur [1]. Surgical drainage with construction of a window is often needed. In patients with thick, purulent effusions and dense adhesions, extensive pericardiectomy may be required to achieve adequate drainage and to prevent the development of constriction. Early surgical drainage may also help prevent late constriction. Intrapericardial streptokinase has been administered to selected patients with purulent or loculated effusions and may obviate the need for a window [9]. The prognosis of bacterial pericarditis is poor with survival in the range of 30%, even in modern series [3].
Pericardial involvement in systemic autoimmune and autoinflammatory diseases
Approximately 5-11% of patients with acute pericarditis may have a systematic autoimmune disease [1]. Acute pericarditis could be the first manifestation of systemic lupus erythematosus. Pericardial involvement is common in Sjögren’s syndrome, rheumatoid arthritis and sclerodermia, but may also be present in systemic vasculitis, Behçet’s syndrome, sarcoidosis and inflammatory bowel diseases. The treatment is especially targeted to the control of systemic disease [7]. The insignificant response to colchicine and the need for adjunctive immunosuppressive agents are clues to the possible presence of autoinflammatory disease [16]. In some of these conditions, anti-IL or anti-TNF agents may be considered.
Radiation pericarditis
Chest radiation is an important cause of pericardial disease [1]. Soon after radiation, the patient may develop acute pericarditis with or without effusion. Recommendations for the prevention and management include radiation therapy methods that reduce both volume and dose of cardiac irradiation whenever possible, and consideration for pericardiotomy due to radiation-induced constrictive pericarditis [3]. The outcome of pericardiotomy is not satisfactory other than when performed for constrictive pericarditis of other causes because of co-existing myopathy.
Drug-related acute pericarditis and pericardial effusion
Pericardial reactions to drugs are rare. Pericardial damage has been associated with 'serum sickness' by blood products or foreign antisera, venoms, foreign substance reactions by direct pericardial applications (e.g. talc, magnesium silicate), silicones, tetracyclines, sclerosants and iron in ß-thalassaemia [1]. Management is based on discontinuation of the causative agent and symptomatic treatment [7]. The use of heparin and anticoagulant therapies is a possible risk factor for the development of a worsening or haemorrhagic pericardial effusion that may result in cardiac tamponade. In a study of 274 patients with acute pericarditis or myopericarditis, the use of heparin or other anticoagulants was not associated with an increased risk of cardiac tamponade [2]. On the other hand, in the setting of co-existing pericardial effusion, full anticoagulation may be a risk factor for tamponade and complications [20].
Conclusion
Initial management of acute pericarditis should be focused on screening for specific causes which will determine the choice of therapy. Hospital admission is recommended for high-risk patients with acute pericarditis. Colchicine use is a first-line therapy for acute pericarditis as an adjunct to aspirin/NSAIDs therapy for three months. Corticosteroids are not recommended as first-line therapy for acute pericarditis as they appear to encourage recurrences. Serum CRP should be considered to guide the treatment length and assess the response to therapy. Evaluation of response to anti-inflammatory therapy is recommended after one week.