

















Background
The term “white-coat hypertension” was coined many years ago to describe a subgroup of untreated individuals with persistently elevated office but normal ambulatory blood pressure values [1]. Compared to subjects with elevated blood pressure both in the clinic and during 24-hour monitoring, those with white-coat hypertension were more likely to be female, younger, less obese, and more recently diagnosed with hypertension.
This clinical condition, also termed as “isolated clinic hypertension”, is frequently diagnosed in current clinical practice. Its prevalence depends on the demographic and clinical characteristics of subjects as well as on the methods (ambulatory or home blood pressure measurement) and blood pressure cut-offs used to define normal out-of-office values. However, the majority of clinical studies have reported that white-coat hypertension accounts for up to 25-30% of individuals attending out-patient hypertension centres [2]. A recent sub-analysis of data collected by the Spanish Ambulatory Blood Pressure Monitoring Registry, aimed at investigating the prevalence and reproducibility of hypertension phenotypes defined by combined clinic and 24-hour blood pressure measurements in about nine hundred untreated patients, showed that white-coat hypertension was detectable in about one fourth of cases [3]. In the Pressioni Arteriose Monitorate E Loro Associazioni (PAMELA) study, an epidemiologic study designed by our group and aimed at determining normal values of home and ambulatory blood pressure in the general population, white-coat prevalence ranged from 9% to 12%, depending on whether out-of-office normotension was defined by home blood pressure or 24-hour ambulatory blood pressure monitoring, respectively [4].
Years of investigation have shown that white-coat hypertension cannot be regarded as a clinical entity of “innocent” nature, but rather as a condition associated with a greater cardiovascular risk, a finding which retains important clinical implications.
Risk of future hypertension
Increasing evidence supports the notion that white-coat subjects are at greater risk of developing a sustained hypertensive state over the years. In the PAMELA population, we identified individuals with white-coat hypertension based on in-office and out-of-office (24-hour monitoring and home) blood pressure measurements and by detecting new-onset sustained hypertension over a long-term follow-up of 10 years [5]. The condition of white-coat hypertension was identified by combined office blood pressure >140/90 mmHg and mean 24-hour values <125/79 mmHg or home blood pressure <132/82 mmHg. At baseline, a total number of 225 (16%) participants were classified as white-coat hypertensives. At follow-up ten years later, 43% of them had progressed to sustained hypertension. As compared to normotension, the risk of developing sustained hypertension was 2.5-fold higher for white-coat hypertension, even after adjustment for age and sex. Similar results were obtained when this clinical condition was identified by home blood pressure criteria. More recently, the risk of progressing from white-coat to sustained hypertension has been assessed in a nationwide unselected population sample of 944 participants living in Finland [6]. During the 11-year follow-up, the rate of progression to sustained hypertension gradually increased from normotension (18%) to white-coat hypertension (52%) and masked hypertension (73%) as well. In subjects displaying white-coat hyeprtension, the relative risk for developing sustained hypertension was almost three times greater than the one detected in the normotensive group, a value almost superimposable to the one described in the PAMELA population.
Cardiometabolic risk
In the past few years, a large body of evidence has accumulated on the association between white-coat hypertension and a variety of factors which contribute to the overall cardiovascular risk profile determination. Compared to normotensive individuals, subjects with white-coat hypertension display higher serum cholesterol, triglycerides, uric acid and glucose values, increased waist circumference and body mass index as well as a greater prevalence of metabolic syndrome [7]. Metabolic alterations in combination with elevated office blood pressure and increased blood pressure variability contribute to the development of subclinical target organ damage at cardiac, vascular and renal level. Finally, the risk of progressive impairment of glucose metabolism (i.e., incidence of new-onset glucose intolerance and diabetes mellitus) has been reported to be significantly greater in white-coat subjects than in truly normotensive subjects. In the PAMELA population, the increase in plasma glucose levels and the incidence of new-onset diabetes (plasma glucose >126 mg/dl or use of antidiabetic drugs) over a 10-year period were significantly greater in individuals with white-coat hypertension than in normotensives and similar to those observed in sustained hypertensives [4,5,7].
Target organ damage
Accumulating evidence focusing on the association between white-coat hypertension and subclinical target organ damage suggests that the risk conveyed by this condition is intermediate between normotension and sustained hypertension. Results of recently performed meta-analyses provide evidence that white-coat hypertension is characterised, at cardiac level, by an increase in left ventricular mass index, a reduction in early to late mitral flow ratio (an index of left ventricular distensibility) and by greater values of left atrial diameter [8]. Target organ damage does not appear to be confined to the heart but it affects the vascular region as well. Indeed, results of a recent meta-analysis show the presence of subclinical carotid damage, as assessed by carotid ultrasonography, in untreated white-coat hypertension [9], with evidence that common carotid intima media thickness undergoes a progressive increase from the normotensive state to white-coat hypertension and sustained hypertension.
Less information is available about large artery stiffness, subclinical renal damage and retinal alterations in white-coat hypertension, although an augmented pulse wave velocity, a greater extent of early renal damage, as assessed by microalbuminuria, and grade 1 and 2 retinopathy have been reported in some studies.
Risk of cardiovascular events
The relationship between white-coat hypertension and the incidence of cardiovascular events has been examined consistently in a number of clinical studies and meta-analyses. In the early investigations, the risk of cardiovascular morbid or fatal events in white-coat hypertensives was reported to be similar to that of normotensive subjects. However, more recent meta-analyses have shown that incident cardiovascular disease in white-coat hypertensives is intermediate between normotensive and sustained hypertensives. This confirms the results of the International Database of HOme blood pressure in relation to Cardiovascular Outcomes (IDHOCO), a prospective registry totalling 6,458 participants from five populations, followed for more than eight years, showing a higher cardiovascular risk in white-coat hypertensives than in their normotensive counterparts [10].
Recently, the PAMELA study has provided novel findings on the risk of cardiovascular and all-cause mortality assessed over a 16-year follow-up period (the longest follow-up period available in studies performed in white-coat hypertension) in stable and unstable white-coat hypertensives individuals, i.e., subjects displaying normal ambulatory blood pressure values associated with persistent or non-persistent office blood pressure elevation at two consecutive visits, respectively [5]. Data were compared with those from a stable true normotensive group (i.e., persistently normal office and ambulatory blood pressure). Compared to the normotensive group, the risk of cardiovascular and all-cause death did not differ in unstable white-coat hypertension, whereas in the stable form of the clinical condition the risk was increased even after adjusting for confounders (Figure 1). These data suggest that only when office blood pressure is persistently elevated is the condition of white-coat hypertension associated with an augmented long-term mortality risk.
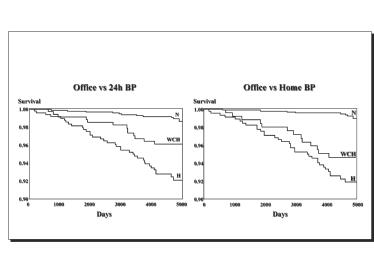
Figure 1. Survival curves of normotensive subjects (N), white-coat hypertensives (WCH) and sustained hypertensives (H) in the follow-up of the PAMELA study.
Data are shown according to the diagnosis of WCH based on ambulatory (left) or home (right) blood pressure (BP) measurement.
Data modified from Ref 4.
Therapeutic implications
No randomised intervention study has prospectively evaluated whether antihypertensive treatment may exert favourable effects on cardiovascular morbidity and mortality in white-coat hypertensive patients. However, recommendations issued by the 2013 European Society of Hypertension and the European Society of Cardiology Guidelines [2] indicate that evaluation of total cardiovascular risk, based on estimation of concomitant risk factors, target organ damage and comorbidities, is essential for the decision about treatment. In white-coat hypertensives without additional cardiovascular risk factors, intervention may be limited to effective lifestyle changes, such as regular aerobic physical activity, weight loss, reduction of salt intake and smoking cessation. This approach has to be associated with a close clinical and laboratory follow-up, including regular home blood pressure measurements and periodical ambulatory blood pressure monitorings. This is because, as mentioned above, white-coat hypertensives display an increased risk of developing metabolic abnormalities (i.e., metabolic syndrome or diabetes) and of progressing to sustained hypertension.
On the other hand, in white-coat hypertensive individuals at high or very high cardiovascular risk, due to the presence of multiple risk factors, type 2 diabetes mellitus, renal dysfunction, any prognostically validated markers of target organ damage and cardiovascular disease, drug treatment may be considered in addition to appropriate lifestyle measures. As cardiovascular risk has been shown to be lower in unstable than in stable white-coat hypertension, antihypertensive treatment is not recommended in the former condition. This is also the case for the stable form of white-coat hypertension without additional risk factors.
Conclusions
The data reviewed in this paper underline the importance of the clinical detection of white-coat hypertension as well as of its accurate follow-up. Assessment of cardiovascualr risk profile and the presence of target organ damage appears essential because white-coat hypertension is by no means a clinically innocent condition, being frequently associated with metabolic alterations, asymptomatic organ damage and risk of cardiovascular events. Although evidence-based data on the therapeutic management of white-coat hypertension are still lacking, the 2013 European Society of Hypertension/European Society of Cardiology Guidelines [2] suggest that antihypertensive drug treatment in white-coat hypertension should be restricted to high or very high risk patients. In order to establish the beneficial effects of blood-lowering interventions in this condition, properly designed, randomised outcome-based trials are needed.