
Background
Although shock delivery by implantable cardioverter-defibrillators (ICD) is a life-saving measure in cases of ventricular tachyarrhythmia, there have been a few notable effects since it was first discovered in the 80's:
- In 1988, external defibrillation was shown to lead to energy-dependent macroscopic myocardial damage and to short-term reduction of systolic left ventricular function in an animal model. (1)
- Ten years later, a decrease of 10% in cardiac index was also found to be "dose-dependent" after increasing shock energy. (2)
- Recently, microscopic myocardial damage (electroporation) was documented along endocardial (3) and epicardial (4) ICD leads after intracardiac shock delivery.
- Humoral cardiac markers (troponin T, CK-MB and myoglobine) increased significantly after intracardiac defibrillation. (5)
Interestingly, intracardiac shocks during defibrillation threshold (DFT) testing lead to a significant reduction in cardiac index only in patients with a reduced LVEF <30% (6), thus suggesting a loss of systolic function especially in previously damaged myocardium.
In 2008, a correlation was found between ICD shocks and mortality, and was labeled the shock paradox in ICD therapy.
Shock paradox
- Increased mortality in patients with primary preventive ICD implantation: In 2008, the SCD-HeFT subanalysis on 811 patients of the Poole et al. study was the first data to reveal a significantly increased mortality in patients with primary preventive ICD implantation and at least one documented intracardiac shock delivery. (7) Over the median follow-up period of nearly 4 years, this fact endured for both appropriate and inappropriate shocks. When focusing on patients surviving the first 24 hours after their first shocks, an increase in all-cause mortality was still observed for appropriate but not for inappropriate shocks. Interestingly, patients with definitely appropriate (with or without inappropriate) shocks had a lower median LVEF (20% EF) than patients with exclusively inappropriate shocks or without any shock (25% EF). The most common cause of death among patients with any ICD shock was progressive heart failure.
- Patients treated with intracardiac shock showed increased mortality: In 2010, a meta-analysis of 4 prospective trials (PainFREE I + II, EMPIRIC and PREPARE) investigating the prevention of ICD shocks by preferential anti-tachycardia pacing (ATP) pooled the data from 2,100+ patients: (8) ventricular tachyarrhythmia treated by ATP had no impact on mortality when compared to patients without ventricular arrhythmia, whereas patients treated with intracardiac shock showed increased all-cause mortality, when compared to those without documented shock. In patients with only inappropriate shocks, this deleterious effect was no longer found.
- Negative effect of appropriate shocks on survival is only evident within the first 4 years after ICD implantation: A smaller single center analysis of 561 patients with heart failure and primary preventive ICD observed the clinical outcome over a median follow-up period of 4 years. (9) The authors concluded that the negative effect of appropriate shocks on survival is only evident within the first 4 years after ICD implantation. Appropriate shocks after the median follow-up period and inappropriate shocks occurring at any time revealed no impact on survival. Remarkably, the deleterious effect of intracardiac shocks was seen only in patients with ischemic heart failure, supporting the theory of higher mortality based on the underlying cardiac disease.
- The adverse prognosis after first shock appears to be more related to the underlying arrhythmia than to an adverse effect from the shock itself: A recent subanalysis of the ALTITUDE registry focused on the "survival by rhythm" in more than 7,400 patients. (10) Significantly higher all-cause mortality was found in patients with appropriate shocks for ventricular arrhythmia as well as in patients with inappropriate shocks caused by atrial fibrillation/flutter, but not those with inappropriate shocks due to other supraventricular tachycardia, noise/artifacts or oversensing. The authors concluded that "the adverse prognosis after first shock appears to be more related to the underlying arrhythmia than to an adverse effect from the shock itself". Unfortunately, this manuscript didn't provide any data on heart failure parameters such as LVEF or NYHA class. Nevertheless, a correlation between mortality and heart failure may be presumed, as ventricular tachyarrhythmia and atrial fibrillation are well known to be more frequent in patients with reduced left ventricular function.
Accelerated ventricular tachyarrhythmia and mortality
Accelerated tachyarrhythmia was associated with significantly higher all-cause mortality: Our own single center analysis on a collective of 1,170 ICD patients over a mean follow-up of 5 years was the first to focus on accelerated ventricular tachyarrhythmia, defined as acceleration (or induction) of a ventricular arrhythmia with a decrease of 10% of the initial cycle length caused by ATP or shock delivery (11). Indeed, in previous publications, the incidence of accelerated ventricular arrhythmias ranged between 1% and 5% within follow-up periods of 2 years maximum. (12-16) Acceleration was documented in 8.5% of all patients and in 17% of patients with documented ATP during this longer follow-up period. Almost all ventricular accelerations were induced by predominantly appropriate ATP (97%) and were in the end, terminated with a shock (99%). Occurrence and recurrence of accelerated tachyarrhythmia were significantly correlated with reduced systolic left ventricular function (LVEF <40%). Most notably, accelerated tachyarrhythmia was associated with significantly higher all-cause mortality. In the multivariable analysis, accelerated ventricular tachyarrhythmia and LVEF <40% were independent predictors for all-cause mortality. In patients with documented ATP, acceleration was an independent mortality predictor as well. Therefore, we found once more a significant correlation between shock delivery and mortality.
However, progressive deterioration of systolic heart failure was likely to be the underlying cause for increased mortality in ICD patients (see next paragraph). The detailed interrelations we found in our collective are summarised in the following figure.
Figure: Parameters with influence on all-cause mortality in patients with ICD (provided by author from reference 11).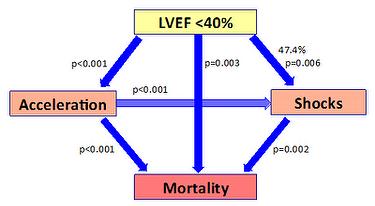
Local injury currents
Patients with stable heart failure NYHA-class I-III revealed local injury currents: A recent investigation on DFT testing in 310 patients with stable heart failure NYHA-class I-III revealed local injury currents (LIC) in the post-shock intracardiac ECG as a clue for pre-damaged myocardium. (17) These LIC are late-potential-like abnormalities of the right ventricular ECG. First, the presence of LIC during DFT testing resulted in a significantly higher adverse event rate (i.e. death, or hospitalisation for deterioration of heart failure). Remarkably, a significant correlation between a higher event rate and the occurrence of ICD shocks was only found in patients with documented LIC. On the other hand, a missing LIC leads to an identical adverse event rate in patients with or without ICD shock.
Thus, local injury currents reflecting a pre-damaged myocardium in patients with progression of systolic heart failure might be the missing link between ICD shock delivery and increased mortality.
Conclusion
The presented "shock paradox" is a chicken-and-egg question in cardiology: can ICD shocks be lethal in the long term, or, are patients with a higher risk of death supposed to undergo shocks?
Intracardiac shocks are saving lives in cases of ventricular tachyarrhythmia, but a significant correlation between shocks and mortality was reported in several studies on ICD therapy. In conclusion, shock delivery is most likely a surrogate parameter, reflecting higher all-cause mortality based on progressive deterioration of the underlying chronic heart failure with reduced ejection fraction.