















Background
Mutations in SCN5A have been implicated in a multitude of inherited cardiac disease with different electrophysiological profiles (1). Gain of function mutations have been associated with long QT syndrome, while loss of function mutations with Brugada syndrome, progressive conduction disease, and sick sinus syndrome (2). Occasionally, the same SCN5A mutation may present with different clinical phenotypes within the same family.
Case Presentation
A 12-year-old boy admitted to our outpatients’ clinic after the occurrence of a sudden cardiac death in a family member.
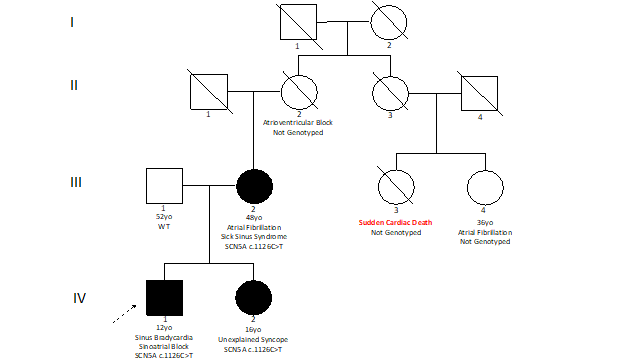
His family history revealed the presence of several cases of cardiac conduction disease (Figure 1). His mother (48-year-old) was affected by sick sinus syndrome and was implanted with a pacemaker after the occurrence of several episodes of symptomatic sinus bradycardia and paroxysmal atrial fibrillation with slow ventricular rate. His grandmother was affected by second-degree atrioventricular block Mobitz type I. His sister (16-year-old) referred two episodes of syncope during physical activity. A mother’s cousin experienced sudden cardiac death at the age of 40 during sleep, while another cousin experienced atrial fibrillation at the age of 30.
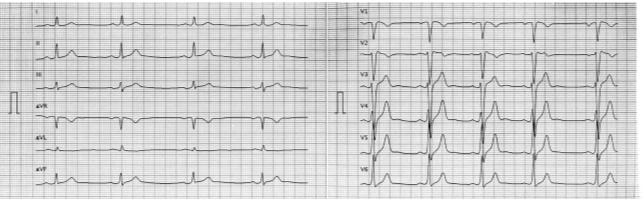
His physical history was unremarkable. The electrocardiogram (ECG) evidence a sinus bradycardia (HR 45 bpm) (Figure 2).
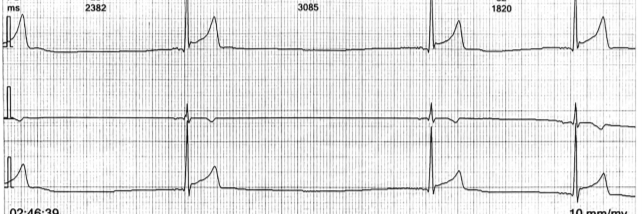
The echocardiography was normal, except for the presence of increased left ventricular trabeculation. 24-hour ECG Holter monitoring revealed the presence of several episodes of second-degree sinoatrial blocks with 16 asymptomatic pauses, with the longest of 2.6 seconds (Figure 3).
The proband underwent genetic testing for genes associated with cardiac conduction disease, which showed a likely pathogenic variant in SCN5A (c.1126C>T; p.Arg376Cys) according to the American College of Medical Genomics (ACMG) criteria. Thus, cascade genetic screening was performed, and genetic testing was positive also in the proband’s mother and sister.
Discussion
We have described the case of a family with cardiac conduction disease due to a disease-causing mutation in SCN5A, a gene responsible for several inherited cardiac disorders. This clinical case emphasizes the importance of genetic testing even in the context of cardiac conduction disorders, especially in the presence of family history. In addition, it highlights the role of molecular cascade screening in detecting affected family members to guide further management.
Cardiac conduction disorder is a genetically heterogeneous disorder, often inherited with an autosomal dominant pattern (3), mostly associated with disease-causing mutations in SCN5A or LMNA (4,5). Thus, the European Heart Rhythm Association (EHRA)/Heart Rhythm Society (HRS)/Asia Pacific Heart Rhythm Society (APHRS)/Latin American Heart Rhythm Society (LAHRS) expert consensus statement on the state of genetic testing for cardiac disease provides specific recommendations in patients with (progressive) cardiac conduction disease (6). In particular, targeted genetic testing is recommended in the index patient with cardiac conduction disease when there is early age of diagnosis or suspicion for laminopathy, especially when there is documentation of a positive family history for cardiac conduction disease.
This family represents an example of the highly variable and complex phenotype associated with SCN5A mutations. Several phenotypes have been associated with loss of function SCN5A mutations, including sick sinus syndrome, conduction disorder, atrial fibrillation, Brugada syndrome, and sudden cardiac death. Except for Brugada syndrome, all these phenotypes were observed in the proband or family members. However, although not diagnostic, the proband showed an ECG pattern (ST-segment elevation ~ 1mm and negative T wave in V1 and V2 leads) similar to those observed in patients with Brugada syndrome. In such cases, the repetition of the ECG with high-lead positioning or a provocative test with sodium channel blockers may be helpful to diagnose a concealed Brugada syndrome.
In conclusion, genetic aetiology may provide prognostic information, guide cascade screening, risk stratification and management. For example, patients with SCN5A pathogenic variants may develop Brudaga syndrome, and the avoidance of certain drugs and the aggressive treatment of fever is generally recommended in these patients to reduce the risk for life-threatening ventricular arrhythmias.

