
Background
Atrial fibrillation (AF) is the most frequent cardiac arrhythmia; moreover, it is associated with significant morbi-mortality. Medical treatment is accompanied with serious drug side effects and often fails to completely preclude complications of AF. Thus considerable advances in developing alternative treatments have been undertaken. Cox pioneered surgical ablation with the Maze procedure and subsequently limited left-atrial ablation lesion sets using alternative energy sources have been described with encouraging results.
Indeed, atrial Fibrillation (AF) is a major public health problem: 4.5 million cases of paroxysmal and persistent AF in the EU were reported in 2004 forming around 1 % of the population. The annual cost of medical treatment per patient is 3000 € totaling 1,86 billion € for the EU. AF leads to a 1.5- to 1.9-fold increase in mortality after adjustment for the preexisting cardiovascular conditions with which AF was related. The goal of AF therapy is to achieve a return to permanent sinus rhythm; however it is interesting to note that the presence of sinus rhythm, but not anti-arrhythmic drugs, is associated with a lower risk of death.
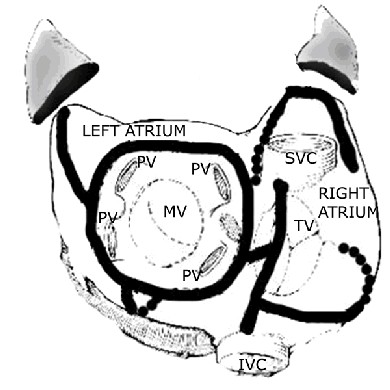
Surgery has played a significant role in the management of AF greatly due to the work of James Cox who set the gold standard with the Maze procedure in which surgical incisions in the atrial wall interrupt the atrial pathways necessary for multiple reentry circuits (figure).
Despite excellent results reported by Cox, the maze procedure is hindered by its technical complexity, risk of significant complications and a non negligible mortality rate and consequently it has been sparsely adopted.
After the work of Haissaguerre showing that left atrial sources of ectopic activity are of particular importance and that arrhythmias originate from ectopic foci in the pulmonary veins up to 94 percent of the time, a less invasive operation including only left atrial lesions was described to facilitate the procedure. Furthermore, surgical incisions were replaced by new surgical approaches employing alternate energy sources to replicate the Cox maze lines of atrial conduction block more quickly.
Alternative Energy Sources
The idea is to perform the Maze procedure by ablating atrial tissue through topical application rather than surgical incisions and suturing i.e., the classical “cut-and-sew technique” permitting faster and less invasive procedures. Again, the main idea is to create lines of intra-atrial conduction block that will :
- stop macroreentrant circuits in the atria,
- isolate the trigger or triggers for AF originating near the pulmonary vein orifices, or
- accomplish both and allow the atria to resume a sinus rhythm
The ideal energy source to achieve such lesions should have the following characteristics:
- achieves lesions quickly and reliably
- yields a full thickness lesion of the atrial wall
- does not damage surrounding tissues
- amenable to off-pump and minimally invasive application
The following are the most common sources of energy employed in clinical use :
Radiofrequency
Radiofrequency produces heat resulting in thermal injury to the atrial tissue. It can be applied to either endocardial or epicardial heart surfaces and can be used off-pump and in minimally invasive procedures for AF. The current state of the art is bipolar radiofrequency clamps that create precise and uniform transmural lesions and give clinical success rates (return to sinus rhythm) of around 85%.
Cryothermy
Cryoablation induces transmural lesions by freezing atrial tissue. Unlike radiofrequency there is no tissue vaporisation or charring and the endocardial surface remains smooth following cryoablation. The benefit of this technique has been illustrated by Cox who initially incorporated cryotherapy into the Cox-Maze III procedure and then performed the entire procedure solely by cryoablation: the ‘cryo-Maze’ procedure. Cryoablation is amenable to minimally invasive procedures.
Ultrasound
High intensity focused ultrasound energy is applied epicardially on the beating heart prior to the concomitant intracardiac procedure to induce ablation lesion sets resulting in deep heating, coagulation necrosis, and conduction block. The device is an array of multiple ultrasound transducers that is used to produce a transmural circumferential left atrial lesion around the pulmonary vein orifices. An additional tool, can be used for the creation of additional linear lesions. Initial clinical results reported excellent early term return to sinus rhythm (80-100%) .
Indications for surgical atrial fibrillation ablation
The current indications are summarised in the consensus statement of the Heart Rhythm Society.
- Symptomatic atrial fibrillation patients undergoing cardiac surgery.
- Selected asymptomatic atrial fibrillation patients undergoing cardiac surgery in whom ablation can be performed with minimal risk.
- Stand-alone surgery should be considered for symptomatic patients who prefer a surgical approach, have failed one or more attempts at catheter ablation, or are not candidates for catheter ablation.
Who to avoid ?
Clinical data have shown that patients with the following characteristics have had the least successful return to sinus rhythm rates after surgical ablation of atrial fibrillation
- enlarged left atrial size (= 60 mm)
- prolonged duration of AF (>10 years)
- electrocardiogram voltage criteria (f Voltage wave in V1 > 0.1 mV)
- advanced age (> 80 years)
Treatment after surgical ablation
Following surgery, a process of reverses atrial modeling “healing” takes place and is frequently accompanied by some form of arrhythmia. Despite the absence of a consensus, antiarrhythmic and anticoagulation drugs are continued for at least three months after the ablation. The criteria for their interruption are based on clinical, ECG and echocardiographic assessment at 3, 6 and 12 months and include the absence of symptoms, return to sinus rhythm and signs of recovered atrial function.
Conclusions
Complexity of the Cox-Maze procedure has led to development of faster, simpler, and less invasive surgical techniques employing alternative energy sources for ablation of AF.
Recent advances and emerging technologies with these techniques have allowed epicardial ablation of atrial tissues on the beating heart and show great promise for application by minimally invasive techniques expanding the indications of surgical ablation for AF.
Patients with paroxysmal AF often have ectopic foci originating around the pulmonary veins and have given best rates of return to sinus rhythm after such procedures. Conversely, patients with large left atria, prolonged duration of AF, advanced age, and associated coronary artery disease have been associated with poorer results.
Figure. The Maze procedure. Black lines delineate surgical incisions in both the right and left atria, encircling the pulmonary veins (PV) and around the coronary artery sinus orifice. The atrial appendages are also excluded.
(MV: Mitral valve, TV Tricuspid valve, SVC: Superior vena cava, IVC: Inferior vena cava)
The content of this article reflects the personal opinion of the author/s and is not necessarily the official position of the European Society of Cardiology.