
“Off-pump” or "beating heart" coronary bypass surgery, also known as OPCAB (for "Off-Pump Coronary Artery Bypass), differs from conventional Coronary Artery Bypass Grafting (CABG) in that the cardiopulmonary bypass pump (extracorporeal circulation) is not employed.
1 - Benefits
Cardiopulmonary bypass and cardioplegia provide :
• a motionless field which facilitates manipulation of the heart,
• stabilises the anastomotic site guaranteeing the quality of the anastomosis, and
• providing myocardial protection during cross-clamping.
However, blood contact through the cardiopulmonary bypass circuit for prolonged periods induces a systemic inflammatory response and impaired hemostasis.
Biologically, on pump CABG has been shown to produce a more significant elevation of the following biochemical, cellular, and molecular inflammatory markers as compared to OPCAB:
• Complement, activated through the classical and alternate pathways [1,2]
• Tumor necrosis factor a, C-reactive protein, elastase [3]
• Interleukin-6, interleukin-8, interleukin-10 [3]
• Leukocytes [3]
• Urinary hypoxanthine, xanthine and malondialdehyde as markers of oxidative stress [4]
• Disturbances in hemostasis after on pump CABG have been demonstrated by lower platelet counts, lower plasminogen and higher
• D-dimer levels after surgery [5].
On-pump CABG is also associated with
• Microembolisation of gas and particles from blood constituents and lipids as they are cycled through the cardiopulmonary bypass circuit [6].
The development of OPCAB was based on decreasing the incidence and/or severity of these adverse outcomes by eliminating extracorporeal circulation. Clinically, OPCAB has indeed shown improved outcomes with benefits including:
• Reduced inflammatory response
• Lesser renal dysfunction [7,8]
• Reduced incidence of stroke [9,10] and cognitive problems [11]
• Lesser coagulopathy and blood transfusion requirement
• Reduced morbidity and mortality [12,13]
• Reduced length of intensive care and hospital stay
2 - Indications
Having passed a significant learning curve (for the surgeon, anesthetist, and theatre staff), multiple bypasses by OPCAB covering all coronary territories are possible with current technology including stabilising devices and intracoronary shunts.
There are two essential techniques available in OPCAB depending on the number and location of the coronary vessels that need to be bypassed.
The MIDCAB approach is performed through a mini thoracotomy mainly for anteriorly located single or two-vessel disease.
The midline sternotomy approach as for conventional CABG.
In general, indications for OPCAB include:
• Coronary artery disease requiring surgical revascularisation
• High risk or contraindications for cardiopulmonary bypass and aortic cross-clamping:
• Severely atheromatous or heavily calcified aorta
• Aortic disease with risk of dissection, rupture or embolisation
• Poor quality target vessels including intramyocardial vessels, diffusely diseased vessels and calcified coronary vessels
• Hemodynamic instability
• Impaired left ventricular function
• Recent myocardial infarction
• History of transient ischemic attacks or cerebrovascular accidents
• Impaired renal function or need for dialysis in patients with chronic renal failure
• Patients who refuse blood transfusions
• Elderly patients, patients with respiratory problems or other systemic disease considered high risk surgical patients because of their reduced functional capacity and the presence of co-morbidities.
Figure 1 provides a decision-making algorithm to choose between on-pump and off-pump approaches [14].
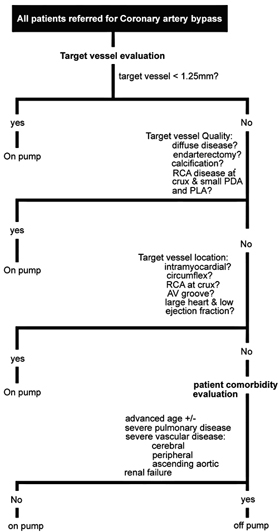
Figure 1. Decision-making algorithm (AV = atrioventricular; PDA = posterior descending artery; PLA = proximal left ascending artery; RCA = right coronary artery) Reprinted from Annals of Thoracic Surgery, 81,Brown JM, et al. Off-Pump Versus On-Pump Coronary Artery Bypass Grafting in Consecutive Patients: Decision-Making Algorithm and Outcomes: 555-561, Copyright (2006), with permission from the Society of Thoracic Surgeons.
The content of this article reflects the personal opinion of the author/s and is not necessarily the official position of the European Society of Cardiology.