It is essential that cardiologists be open to collaborating tightly with other disciplines, and diabetologists especially- as recommended by the previous 2007 guidelines on diabetes, pre-diabetes and cardiovascular diseases, yet our responsibility remains managing our patients and cardiovascular health will not improve if we leave our responsibility to other professionals.
With nearly half of outpatients attended by practising cardiologists either diabetics, pre-diabetics, or developing or unveiling type 2 diabetes in the near future, this is no small task.
Indeed, prevalence of diabetes mellitus (DM) and pre-diabetic states- defined by an elevated blood glucose level -whether fasting after meals or a glucose load (1)- is high and still rising in Europe. Both diabetes mellitus (DM) and pre-diabetic states are risk factors for cardiovascular (CV) disease. Their emergence starts many years before clinical events appear, with macrovascular (or CV) involvement and the microvascular complications that follow developing silently, in parallel with the progression from pre-diabetic status to type 2 DM.
I - Risk, investigations and targets
Main mechanisms linking diabetes mellitus (DM) and cardiovascular (CV) disease include insulin resistance, endothelial dysfunction, dyslipidemia, and a pro-coagulant state. (2) It is recognised that general and DM-specific scores for assessing CV risk (such as Framingham, SCORE, DECODE, PROCAM or REGICOR in patients without DM or UKPDS, NDR, the UKPDS or ADVANCE in patients with DM) are at best limited in value for patients with DM or pre-diabetes.
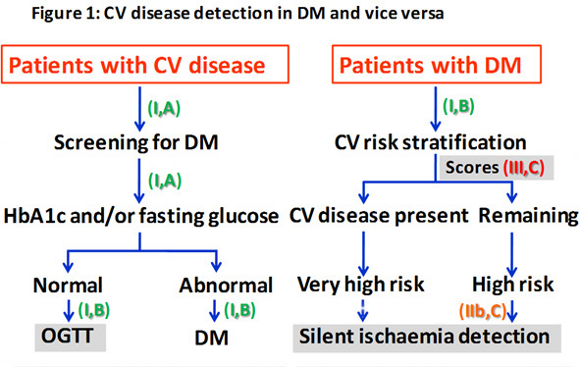
European guidelines have simplified CV risk stratification to only two categories: 1) very high risk if CV disease is already present and 2) high risk in the remaining patients with type 2 DM or pre-diabetes.
Cardiovascular disease should be investigated in patients with DM or metabolic syndrome, yet silent ischaemia needs not to be screened for, as had previously been stated, in all patients with DM.
Similarly, stress testing is only recommended in patients who are symptomatic or who have an especially high risk due to the presence of other risk factors.
On the other hand, disorders of glucose metabolism should be investigated in all patients with a CV event. Glycated haemoglobin (A1c), fasting plasma glucose, or both are recommended as screening procedures. In all cases in which other parameters are normal, an oral glucose tolerance test is recommended for its high predictive value for CV events (Figure 1).
Lifestyle adjustment is the first and most powerful therapy for preventing CV disease in patients with type 2 DM or pre-diabetic states. The main components of adequate lifestyle for that purpose are to: a) stop and/or avoid smoking; b) maintain a normal weight; c) consume a healthy diet, which includes limiting salt, alcohol, and saturated fats, as well as limited sugar or sugar-like foods, and increasing monounsaturated and fiber intake; and d) increasing physical activity, both aerobic and resistance exercises.
Effective glucose control reduces microvascular complications in type 1 and type 2 DM. It also reduces CV events in patient with type 1 DM, but not as consistently in recently diagnosed type 2 DM, and almost not at all in long-standing type 2 DM (elderly patients). Therefore, ESC guidelines recommend the standard glycaemic target (HbA1c less than 7%) in most cases and a tighter target (6.5 to 6.9%) for selected patients, i.e, those younger, with DM of short duration, and those without co-morbidities.
Blood pressure control has also been simplified. (3) Diastolic pressure targets should be 85 mm Hg or less for all patients with DM. Systolic target is set at 140 mm Hg for all patients, except in those with nephropathy and proteinuria in whom systolic target should be lowered to less than 130 mm Hg.
II - Drug treatment
Recommended lipid-lowering strategies are in accordance with the 2011 ESC guidelines on dyslipidaemias. (4) Main treatment target should be LDL-cholesterol and therefore statins are the principal drugs to achieve recommended values: less than 1.8 mmol/L (70 mg/dL) for patients with DM and very high risk, and less than 2.5 mmol/L (100 mg/dL) for those at high risk. Non-HDL-cholesterol is considered a secondary objective and the recommended values are 2.6 mmol/L (100 mg/dL) and 3.3 mmol/L (130 mg/dL), respectively.
The debate over aspirin in primary prevention for patients with DM continues. Guidelines recommend aspirin only in patients with high risk and on an individual basis. In secondary prevention however, aspirin (or clopidogrel in cases of intolerance) is indicated indefinitely, and both drugs combined during the first year after a coronary event. Other antiplatelet drugs (prasugrel, ticagrelor) in association with aspirin have shown better performance during the first year after an acute coronary syndrome.
Medical management of ischaemic heart disease is no different in patients with or without DM. Optimal medical treatment is the preferred modality for patients with stable coronary disease. Classical indications for beta-blockers, angiotensin converting enzyme inhibitors or angiotensin receptor blockers, statins, and antiplatelet drugs are summarised in the guidelines.
Recommendations regarding coronary revascularisation differ according to whether revascularisation regards patients with DM or without. In patients with DM, artery bypass surgery is preferred over percutaneous coronary intervention in complex multivessel disease, aiming for complete revascularisation with arterial bypass grafts. When percutaneous revascularisation is necessary in these patients, drug-eluting stents rather than bare-metal stents are preferred to reduce the risk of target vessel re-interventions.
Drug treatment for heart failure in patients with DM includes the classical triad : angiotensin converting enzyme inhibitor, betablocker, and diuretic if necessary. An aldosterone antagonist should be added in patients with ejection fraction less than 35% and persistent symptoms. Ivabradine may be added for symptomatic patients with low ejection fraction, sinus rhythm, and a high resting heart rate.
It is recommended to investigate for the presence of silent paroxysmal atrial fibrillation since atrial fibrillation is highly prevalent in diabetic patients. Rules for anticoagulation do not differ from the current recommendations: vitamin K antagonists or novel oral anticoagulants are both considered equal alternatives for embolic prevention.