
Introduction
Over the past 40 years there have been significant changes in the disease pattern around the world. At a recent press conference, World Health Organization (WHO) Director-General, Dr Margaret Chan, reported unprecedented progress against neglected tropical diseases. Millions of people have been rescued from disability and poverty, thanks to one of the most effective global partnerships in modern public health. Non-communicable diseases (NCDs) have replaced the earlier global threats to health such as undernourishment, malaria, HIV and TB. They have become the main causes of premature death.
According to the WHO, 40 million people die annually due to a NCD, which amounts to 70% of all global deaths, and 17 million people die before the age of 70. NCDs are increasing significantly in low- and middle-income countries: 87% of premature deaths occur in low- and middle-income countries. Together, cardiovascular diseases (CVDs), cancer, respiratory diseases and diabetes mellitus account for 81% of all deaths in NCDs. It is expected that the global burden of NCDs will increase by 17% by 2025.
Cardiovascular disease is the foremost NCD killer: in 2015 there were more than 400 million individuals living with CVD and nearly 18 million CVD deaths worldwide according to the most recent Global Burden of Disease study, an international consortium of more than 2,300 researchers in 133 nations in 2015 [1]. Mortality has been reduced: over the past two decades, the age-standardised death rate from CVD dropped globally, mainly driven by improvements in high-income countries. Worldwide, there were about 393 CVD deaths per 100,000 which has come down to 286 deaths per 100,000 in recent years.
NCDs have a huge economic impact: the recent OECD report (Health at a Glance, Europe 2016) reports that the economic loss due to premature death from NCDs amounts to 115 billion euros annually [2]. This report indicates several critical actions that are urgently required: fighting obesity is one of the prime targets for political action, alongside reducing the use of tobacco and alcohol.
NCDs are caused largely by four modifiable risk factors: tobacco use, unhealthy diet, physical inactivity, and harmful use of alcohol. According to the WHO, 80% of premature CVD can be prevented through action against these four behavioural factors.
Causes of CVD
Initially, smoking was the main cause of premature CVD but, as the prevalence of tobacco use has been gradually decreasing over the past years, being overweight and obesity have grown to become a veritable global health threat. Yet, in spite of this worldwide progress since the publication of the 2005 WHO Framework Convention on Tobacco Control, not all key demand-reduction measures have been fully implemented at a national level. Thus, further preventive action is needed to reduce tobacco use even more [3].
Since 2015 there are more overweight or obese people than underweight people worldwide. Globally, the average body weight has increased by six kilograms since 1975. As a consequence, an increase in the prevalence of type 2 diabetes has been reported, not only among middle-aged people but at younger ages as well. The pandemic of diabetes mellitus, a major cardiovascular risk factor, will inevitably lead to even more cardiovascular disease-related illness and death. Is this inevitable? Certainly not: as shown in a recent study, individuals who meet behavioural targets, such as the American Heart Association's 2020 impact goals, in terms of dietary intake, physical activity, smoking, blood pressure, cholesterol, and body mass index, are less likely to develop type 2 diabetes [4].
Initiatives at the political level
The development of NCDs has prompted a reaction among politicians worldwide. There are several important initiatives at UN level such as the “25 by 25” recommendation, reducing mortality in NCD by 25% by 2025 and the UN Sustainable Development Agenda aiming (among 17 action points) to reduce NCD mortality by one third by 2030 [5]. In order to translate political ambitions into practical action, the WHO has published a detailed roadmap for preventive action, the Action plan for the prevention and control of NCDs in the WHO European Region [6]. There are many stakeholders involved in this roadmap: one of these is the European Chronic Disease Alliance (ECDA), which is a collaborative effort among 11 major professional organisations including the European Society of Cardiology (ESC), the European Society of Hypertension and the European Heart Network. Its aim is to promote needed and appropriate health legislation in the European Union.
Where is preventive action needed most?
The challenges for NCD prevention, including the battle against premature CVD, vary widely across Europe. Whereas the risk of dying from one of the four main NCDs before the age of 70 is low in some countries (Switzerland 9%, Italy and Sweden 10%, France 11%, Germany 12%), the same risk is up to threefold higher in the eastern European region (Bulgaria 24%, Belarus 26%, Ukraine 28%, Russian Republic 30%). Differences in the prevalence of smoking and of obesity are two of the main explaining factors; however, differences in access to and the quality of medical care play a role as well.
The WHO has an eminent website where concise data on NCDs at national level can be found: http://www.who.int/nmh/countries/en/ (Figure 1). On the website of the European Association of Preventive Cardiology (EAPC), the reader is recommended to visit the “Prevention in your country” page, where the state of preventive cardiology in 37 different countries has been provided by national coordinators for CVD prevention: https://www.escardio.org/Sub-specialty-communities/European-Association-of-Preventive-Cardiology-(EAPC)/Prevention-in-your-country/country-of-the-month
Figure 1. WHO NCD overview for Sweden.
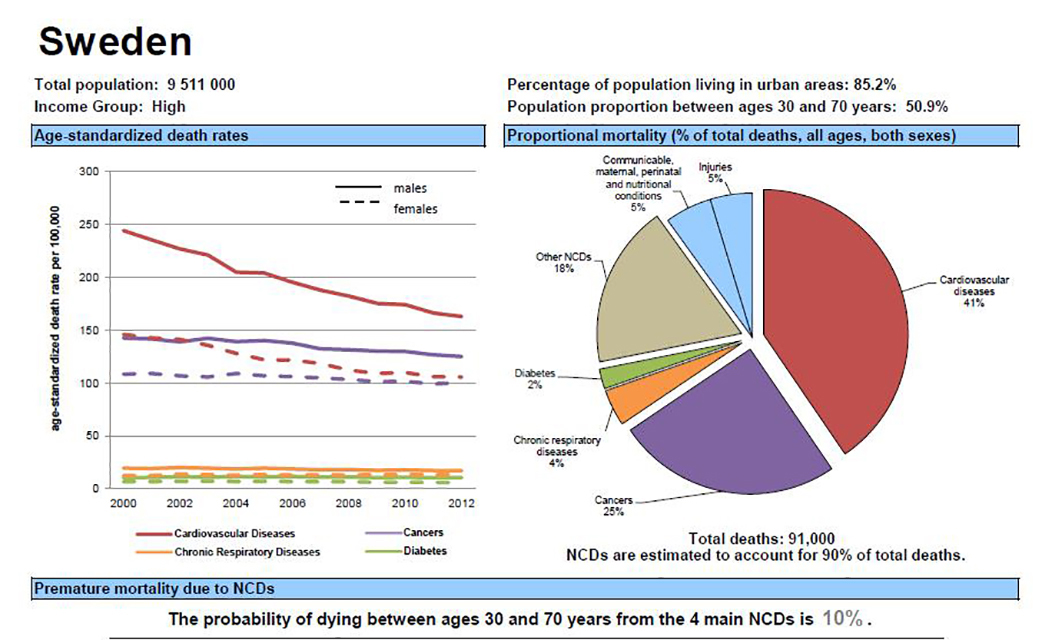
Reprinted with permission from World Health Organisation: NCD country profile 2014: Sweden http://www.who.int/nmh/countries/swe_en.pdf
Scientific rationale for prevention
Is there sufficient scientific evidence to guide preventive action? Over recent decades there have been regularly updated guidelines on CVD prevention from the European Societies’ Joint Task Forces in which the ESC and its daughter branch for prevention (the EAPC) have played a coordinating role. The key target values for prevention are shown in Table I. These guidelines were previously directed to clinical practice but the 2016 guidelines mark an important addition: for the first time evidence-based guidance has been provided for prevention at a population level [7]. One of the target groups for this guidance is health decision makers at different levels. The recommendations include those concerning the use of tobacco, physical activity, nutrition and the use of alcohol, such as the following Class I recommendations:
- Banning smoking in public places is recommended to prevent smoking and to promote smoking cessation. Class I A
- It is recommended to advise parents never to smoke in cars or in private homes. Class I A
- Increased availability and types of school playground spaces and equipment for exercise activity and sports are recommended. Class I C
- Consideration of physical activity when planning new landscaping/buildings or towns is recommended. Class I C
- Elimination of industrially produced trans fats is recommended. Class I A
- Mandatory and simplified harmonised front-of-pack nutrition labelling is recommended. Class I C
- Drink-driving countermeasures are recommended such as lowered blood alcohol concentration limits and “zero tolerance”, random breath testing and sobriety check points. Class I A
- Measures to support and empower primary care to adopt effective approaches to prevent and reduce harmful use of alcohol are recommended. Class I B
Table I. Risk factor goals and target levels for important CVD risk factors.
|
RISK FACTORS |
TARGET |
|---|---|
|
Smoking |
No exposure to tobacco in any form. |
|
Diet |
Low in saturated fat with a focus on wholegrain products, vegetables, fruit and fish. |
|
Physical activity |
At least 150 minutes a week of moderate aerobic PA (30 minutes for 5 days/week) or 75 minutes a week of vigorous aerobic PA (15 minutes for 5 day/week) or a combination thereof. |
|
Body weight |
BMI 20–25 kg/m². Waist circumference <94 cm (men) or <80 cm (women). |
|
Blood pressure |
<140/90 mmHg* |
BMI = body mass index
*Blood pressure <140/90 mmHg is the general target. The target can be higher in frail elderly, or lower in most patients with DM (for further information see chapter 3.a.8, [7]) and in some (very) high-risk patients without DM who can tolerate multiple blood pressure lowering drugs (for further information see chapter 3.a.9, [7]).
Adapted from Piepoli MF, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR), Table 6. With permission from Oxford University Press [7].
Preventive actions
Preventive legislation can be effective: the significant success of the combination of information campaigns on the unhealthy effects of smoking with legislation restricting smoking in public environments, and taxation and rules on advertising, serves as an excellent example [8].
As obesity is becoming the major public health threat in Europe, a similar approach to that which paved the way for the reduction in smoking seen in most European countries over recent decades could be implemented with regard to nutrition. This could be accomplished through a close collaboration among politicians, administrators and representatives of the medical profession as there is an abundance of scientific evidence concerning the beneficial effect of nutrition policies on population health.
Changes at population level in total caloric intake or types of food consumed consistently lead to a decrease in obesity, diabetes and cardiovascular disease [9,10]. Even modest changes can have a considerable impact: for a country such as the UK, reducing intake of industrial trans fatty acids by 0.5% of total energy intake would generate savings of £230m (€267m) a year [11] or even more [12]. A tax on sugar-sweetened beverages could prevent 25,000 adults from becoming overweight or obese in Ireland [13] and over 1.5 million in Germany [14]. Taxing sugar-sweetened beverages would not only prevent overweight and obesity but also dental caries, leading to extra cost savings and reducing socioeconomic inequalities [15]. A reduction in daily salt intake by one gram is cost-effective [16] and, combined with a replacement of saturated by polyunsaturated fat, was estimated to lead to annual savings of €7.5 to €11 million in Finland [17].
Insufficient physical activity is one of the leading risk factors for death worldwide and is a key risk factor for NCD. More than 80% of the world's adolescent population is insufficiently physically active. WHO member states have agreed to reduce insufficient physical activity by 10% by 2025. Physical activity is declining worldwide and this could at least partly be due to reductions in active commuting (walking or cycling) [18]. As a population health-promoting action, active commuting has been recommended as a practical way of incorporating more physical activity into daily life. A meta-analysis of 173,146 participants reported that active commuting was associated with a lower risk of adverse cardiovascular outcomes, especially for women [19]. A recent UK study reported that cycle commuting was associated with a lower risk of CVD, cancer, and all-cause mortality, and that walking commuting was associated with a lower risk of CVD. The authors suggested that initiatives to encourage and support active commuting could reduce risk of death and the burden of NCDs [20].
Conclusion
There is solid scientific guidance both for clinical practice and for decision makers to combat the growing global threat of non-communicable diseases with cardiovascular disease as its main contributor. A further reduction in the use of tobacco, supporting regular physical activity and healthy food choices and limiting the use of alcohol will all have a significant impact on population health. It is time to join hands with all stakeholders to achieve the promise of better global health - the challenge must be faced!