

Introduction
Angina pectoris is a symptom that is fundamental in the training of medical students but still remains an enigma to the most experienced cardiologist. It is the clinical hallmark of myocardial ischaemia and most often perceived as a marker for coronary artery disease (CAD). Understanding the clinic-pathophysiological correlates with this symptom has evolved over the centuries, with a dramatic increase in our knowledge when the epicardial coronary arteries could be imaged via angiography. However, this technology has also made us aware of knowledge gaps, since it is not uncommon to identify patients with angina who have no significant CAD on angiography. Accordingly, other explanations have evolved to explain this puzzling symptom, requiring consideration of functional as well as structural coronary heart disease [1]. Furthermore, our approach to angina has evolved to not merely considering this symptom in isolation but also its impact on patient health. Thus, the health status of patients with angina is an important concept as we move to an era of personalised medicine.
Historical aspects of Angina Pectoris
The term “angina” is derived from the Greek word “ankhone”, meaning “a strangling sensation”, and “pectoris” derived from Latin, referring to the chest. Angina is typically the clinical hallmark of myocardial ischaemia, and usually the result of CAD, although several factors play a role in the pathophysiology of angina. The history of angina begins with Leonardo Da Vinci’s account of coronary artery anatomy in 1511; however, the functional concept of the coronary circulation was not conceived until William Harvey’s description in 1649, as described in his less well-known manuscript “De Circulo Sanguinis in Corde”. However, it was William Heberden, who in 1772 [2], gave the classic clinical description of angina that still has relevance today:
“But there is a disorder of the breast marked with strong and peculiar symptoms, considerable for the kind of danger belonging to it, and not extremely rare, which deserves to be mentioned more at length. The seat of it, and sense of strangling, and anxiety with which it is attended, may make it not improperly be called angina pectoris.
They who are afflicted with it, are seized while they are walking, (more especially if it be up hill, and soon after eating) with a painful and most disagreeable sensation in the breast, which seems as if it would extinguish life, if it were to increase or to continue; but the moment they stand still, all this uneasiness vanishes.”
More than a century later Edward Jenner (the pioneer of the smallpox vaccine) reported the clinicopathological link between angina pectoris and atherosclerotic CAD, through his discovery of advanced changes in the coronary arteries on the autopsy of John Hunter, who presumably died following acute myocardial infarction (AMI). However, further advances were hindered for 150 years until the coronary arteries could be imaged in vivo, with the advent of coronary angiography.
The Angiography Era
Since its inception 50 years ago, coronary angiography has become the benchmark clinical diagnostic technique for imaging and managing structural CAD in contemporary cardiology. Although coronary angiography has certain risks and limitations, its widespread clinical application has revolutionised our understanding of CAD for many patients, but has also demonstrated that our knowledge of ischaemic heart disease is incomplete if only considered on a structural basis. Indeed, as many as 10% of patients with AMI [3] and over 60% [4] of those undergoing elective coronary angiography, do not have evidence of obstructive CAD, so that alternate explanations are required to establish a clinicopathological link. Thus, the coronary circulation must also be studied from a functional perspective with blood vessels considered as “dynamic conduits” rather than structurally “rigid pipes”.
Correlation of angiography findings with angina presentation
As the first reliable in vivo marker for the presence of obstructive coronary lesions, the coronary angiogram provided objective evidence to support the clinical diagnosis of angina pectoris. Initial comparative analyses in the 1960s indicated that obstructive atherosclerosis could be demonstrated in the major coronary arteries in most patients with exertional angina and abnormal exercise electrocardiograms [5]. This “stable angina” syndrome, predictably produced ECG evidence of myocardial ischaemia when myocardial oxygen demand exceeded supply, manifesting as exertional chest pain. In contrast, “unstable angina” typically manifests as rest angina, although it may also present as crescendo angina or mixed pattern angina (episodes of rest and exertional angina), and is attributable to an abrupt reduction in coronary blood flow often with associated thrombosis. In AMI, DeWood’s pioneering early angiographic studies confirmed the presence of an occluded coronary artery in 87% of patients with ST-elevation [6] but was evident in only 26% of patients with non-ST-elevation myocardial infarction. These findings laid the foundations for the “open artery” management strategy in STEMI and the routine use of antithrombotic therapy in all AMI patients.
Although the advent of coronary angiography provided important clinical insights into CAD, it also precipitated clinical enigmas. In 1967, William Likoff presented 15 cases, all female, considered to have unmistakable CAD with typical angina pectoris and electrocardiographic abnormalities; surprisingly none had obstructive CAD [7]. Subsequent studies demonstrated stress-induced myocardial lactate production in both the patients with and without CAD [8], confirming that the chest pain was ischaemic in origin.
Coronary angiography findings and angina characteristics
The American College of Physicians have operationalised the original description of angina pectoris, classifying the symptoms into three categories: typical (definite) angina, atypical (probable) angina, and non-specific chest pain [9] (Table 1). These angina characteristics were evaluated in patients undergoing elective angiography for the investigation of suspected CAD in the Coronary Artery Surgery Study [10]. They observed differences in the prevalence of obstructive CAD (defined as ≥70% stenosis) not only on the basis of angina characteristics but also dependent on gender. Thus, obstructive CAD in men was evident in 93%, 66% and 14% of those with definite angina, probable angina and non-specific chest pain, respectively, whereas the corresponding frequency in women were 72%, 36% and 6%. Thus, the likelihood of obstructive CAD in women with definite angina was significantly less than in men, although the difference was less evident in patients older than 70 years. Therefore, even scrutiny of the chest pain features revealed a significant proportion of patients with classic anginal symptoms who had no evidence of obstructive CAD on angiography, especially amongst women.
Table 1. American College of Physicians angina pectoris criteria.
| Condition | Criteria |
|---|---|
| Typical angina (definite) |
|
| Atypical angina (probable) | Fulfils only two of the typical angina characteristics |
| Non-specific chest pain | Fulfils only one of the typical angina characteristics |
Modified with permission from Diamond et al [9]
The above-mentioned gender difference has stimulated further research, particularly as earlier datasets and conclusions were largely based upon male populations. Importantly, a meta-analysis of 74 studies, concluded that women have a similar or slightly higher prevalence of angina than men [11]. Furthermore, the WISE (Women's Ischemia Syndrome Evaluation) study demonstrated that 57% of women with symptoms suggestive of myocardial ischaemia do not have obstructive CAD on coronary angiography, implicating an alternative mechanism is responsible for the symptoms [12]. Of concern, the WISE study demonstrated that at least half of the women continue to suffer from angina at 12-month follow-up, and also have a higher rate of adverse events compared to asymptomatic women [13].
Angina and coronary vasomotor disorders
The prevalent use of coronary angiography in routine clinical practice has precipitated an increasing interest in functional disorders of the coronary circulation, particularly epicardial coronary artery spasm and coronary microvascular dysfunction. Since coronary angiography enables visualisation of the epicardial coronary arteries it has an important role in the assessment of coronary artery spasm, but a more limited role in the assessment of the coronary microcirculation (except for the coronary slow flow phenomenon).
Epicardial coronary artery spasm
Vasospastic angina is a clinical entity resulting from epicardial coronary artery spasm and should be considered in the differential diagnosis of patients with angina in the absence of obstructive CAD on angiography. An international consensus on the diagnostic criteria for vasospastic angina has recently been published by COVADIS (Coronary Vasomotion Disorders International Study group) [14]. The disorder typically manifests as rest angina (classically in the early morning hours) that is responsive to short-acting nitrates [14]. Ischaemic ECG changes (including ST elevation) may be evident during the anginal episode and are usually transient in nature. The hallmark angiographic finding is intense coronary vasoconstriction producing total or subtotal vessel occlusion. However, spontaneous coronary spasm episodes are seldom captured on angiography and thus require provocative spasm testing. This involves administration of a provocative vasospastic agent (e.g., acetylcholine or ergonovine) during coronary angiography and evaluating if epicardial coronary spasm is induced in association with angina and ischaemic ECG changes.
Coronary microvascular dysfunction
The role of coronary microvascular dysfunction (CMD) as a cause of angina has become more apparent over the past 40 years. Initially described as the cardiological syndrome X (as distinguished from the metabolic syndrome X) in patients with typical exertional angina, abnormal stress ECG test, yet normal angiography and no features of coronary spasm. Subsequently, researchers used other modalities to identify the presence of CMD in patients with angina and normal angiography including impaired coronary flow reserve (microvascular angina), delayed epicardial coronary artery contrast opacification on angiography reflecting increased distal coronary resistance (the coronary slow flow phenomenon), and acetylcholine-provoked chest pain and ischaemic ECG changes in the absence of inducible coronary artery spasm (microvascular spasm). The diagnostic criteria and landmark studies of these CMD disorders are summarised in Table 2. The angina associated with these conditions may mimic the classic Heberden description, but many patients also have unusual characteristics such as prolonged episodes and a variable response to sublingual nitrates. Thus, further evolution in our understanding of angina pectoris will develop with advances in our knowledge of these disorders.
Table 2. Clinical features and landmark research findings in the evolution of coronary microvascular disorders.
| Disorder | Clinical Features | Authors | Landmark research findings |
|---|---|---|---|
| Cardiac syndrome X |
|
Arbogast & Bourassa 1973 | Undertook rapid atrial pacing in patients with exertional angina and obstructive CAD (Group C, n=11) or no CAD (Group X, n=10), demonstrating ischaemic ECG changes and lactate production in both groups. |
| Kemp 1973 | Introduced the term “syndrome X” in the accompanying editorial for the Arbogast and Bourassa paper. |
| Disorder | Clinical Features | Authors | Landmark research findings |
|---|---|---|---|
| Cardiac syndrome X |
|
Arbogast & Bourassa 1973 | Undertook rapid atrial pacing in patients with exertional angina and obstructive CAD (Group C, n=11) or no CAD (Group X, n=10), demonstrating ischaemic ECG changes and lactate production in both groups. |
| Kemp 1973 | Introduced the term “syndrome X” in the accompanying editorial for the Arbogast and Bourassa paper. | ||
| Microvascular angina |
|
Opherk et al 1981 | Initial description of 21 (6 female) patients with exertional angina, normal angiography and abnormal coronary blood flow response to dipyridamole |
| Cannon & Epstein 1988 | Introduced the term “microvascular angina” to describe patients with evidence of impaired coronary blood flow response | ||
| Microvascular spasm |
|
Mohri et al 1998 | Demonstrated microvascular spasm in 29/117 (25%) patients undergoing acetylcholine provocation spasm testing. Confirmed lactate production in these patients, supporting a diagnosis of microvascular spasm. |
| Coronary slow flow phenomenon |
|
Tambe et al 1972 | Examined 6 patients with normal coronary angiography, abnormal resting ECG and strikingly slow passage of contrast medium through coronary arteries. |
| Beltrame et al 2002 | Identified the clinical characteristics of this angiographic phenomenon |
Angina and health status
The introduction of percutaneous coronary transluminal angioplasty pioneered by Gruntzig, followed by the development of intracoronary stents in the mid 1980s, revolutionised the treatment of CAD. Although survival following an acute coronary syndrome has significantly improved, one of the areas in which contemporary cardiology has not been able to meet the patient’s needs is the optimal management of angina, emphasising a significant gap in achieving patient-centred care. An important point of note is the traditional focus by clinicians of “the disease”, whereas patients are focused on “how does this affect my life?”.
Significance of health status
Health status is the level of health of an individual as subjectively assessed by the individual, i.e., how someone feels and how they function in their daily activities. Specifically, health status is defined as the impact of disease on a patient, including symptoms, functional limitation (dependent upon the patient’s expectations, for example, unable to walk a flight of stairs may be perceived as a major limitation by some but not all patients with angina), and quality of life, in which quality of life is the discrepancy between the patient’s actual and desired function [15]. This conceptual model of health status is depicted in Figure 1. The measurement of health status is achieved using standardised questionnaires, such as the Short Form-36 (SF-36). In the case of angina, the Seattle Angina Questionnaire (SAQ) has evolved as the gold standard measure of condition-specific health status. Although health status measures may be viewed as “soft endpoints”, they are developed using rigorous validity and reliability testing. In fact, the SAQ is more reproducible than clinician interpretation of coronary angiography [16]. Furthermore, patient-reported health status been shown to be a significant predictor of mortality and hospitalisation in CAD patients [17], underscoring the importance of this indicator in patient care.
Figure 1. An overview of health status domains in coronary artery disease.
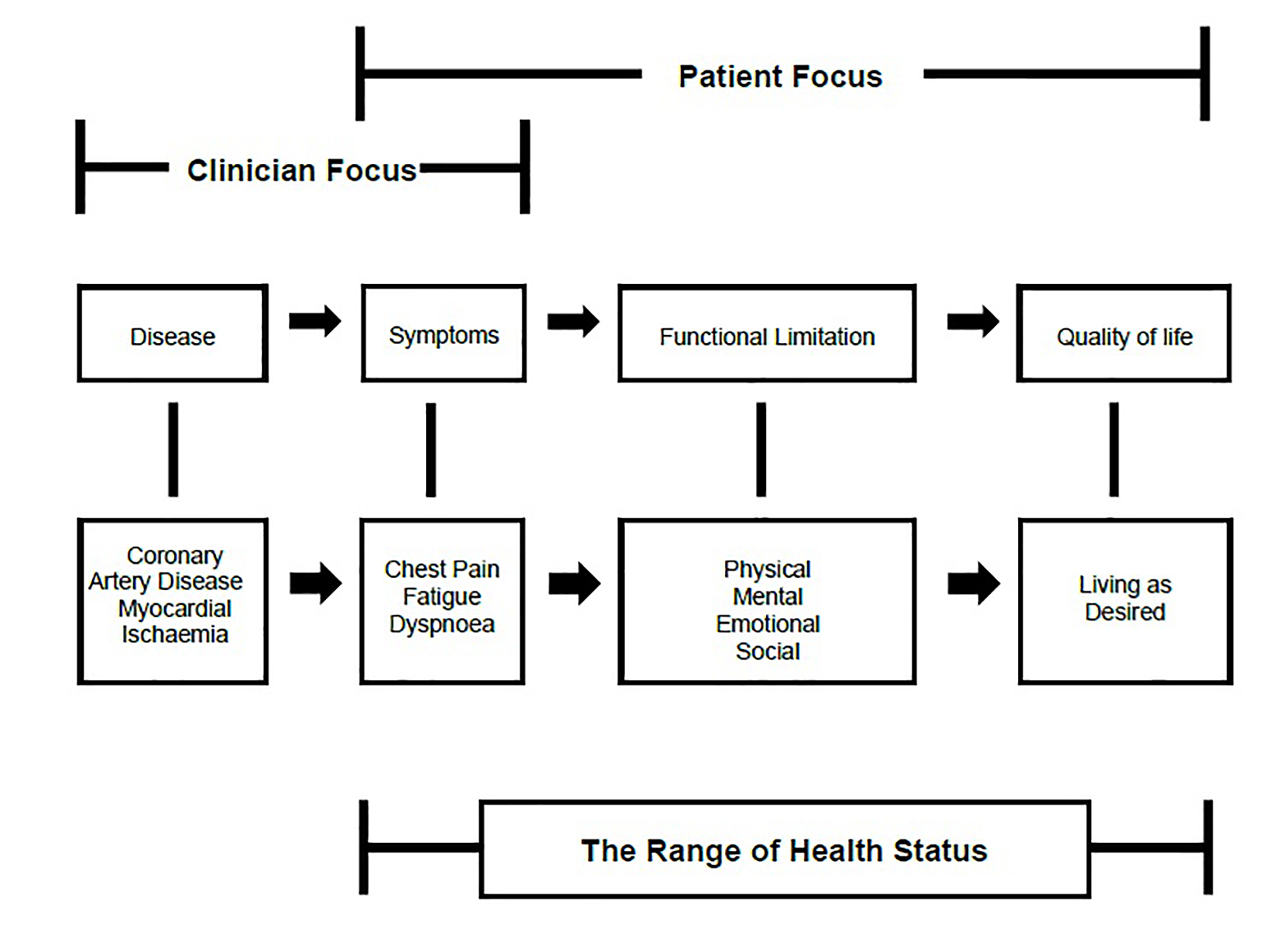
The range of health status domains in coronary artery disease: symptoms, function, and quality of life. Figure adapted with permission from Spertus et al [18] and Wilson and Cleary [19]
Angina symptoms and the impact on health status
The frequency of angina symptoms may be considered an important determinate of health status. The Coronary Artery Disease in General Practice (CADENCE) Study was conducted in an Australian primary care cohort and demonstrated that 29% of stable angina patients report chest pain episodes at least once a week [20]. The patients who reported at least weekly angina also showed more physical limitation and poorer quality of life compared to patients reporting less frequent angina, as shown in Figure 2. Thus, the simple enquiry of how often a patient experiences chest pain provides useful insights into the impact of angina on health status. Interestingly, clinicians reported that 80% of their patients had optimally controlled angina and that 61% had minimal impairment in their physical activity by the angina. In contrast, from the patient-reported health status, only 52% of patients reported being angina-free and only 47% described their angina as not limiting their enjoyment in life. This underscores the importance of patient-reported symptoms since clinicians may not accurately estimate the full impact of the angina on the patient. It is also evident that clinical investigations, such as the angiogram, have a limited role in determining patient health status. Clinical registry data demonstrate that patients undergoing coronary angiography for the investigation of angina have similarly impaired health status regardless of whether obstructive or non-obstructive CAD is revealed [21].
Figure 2. Relationship between angina frequency and patient reported health status indices.
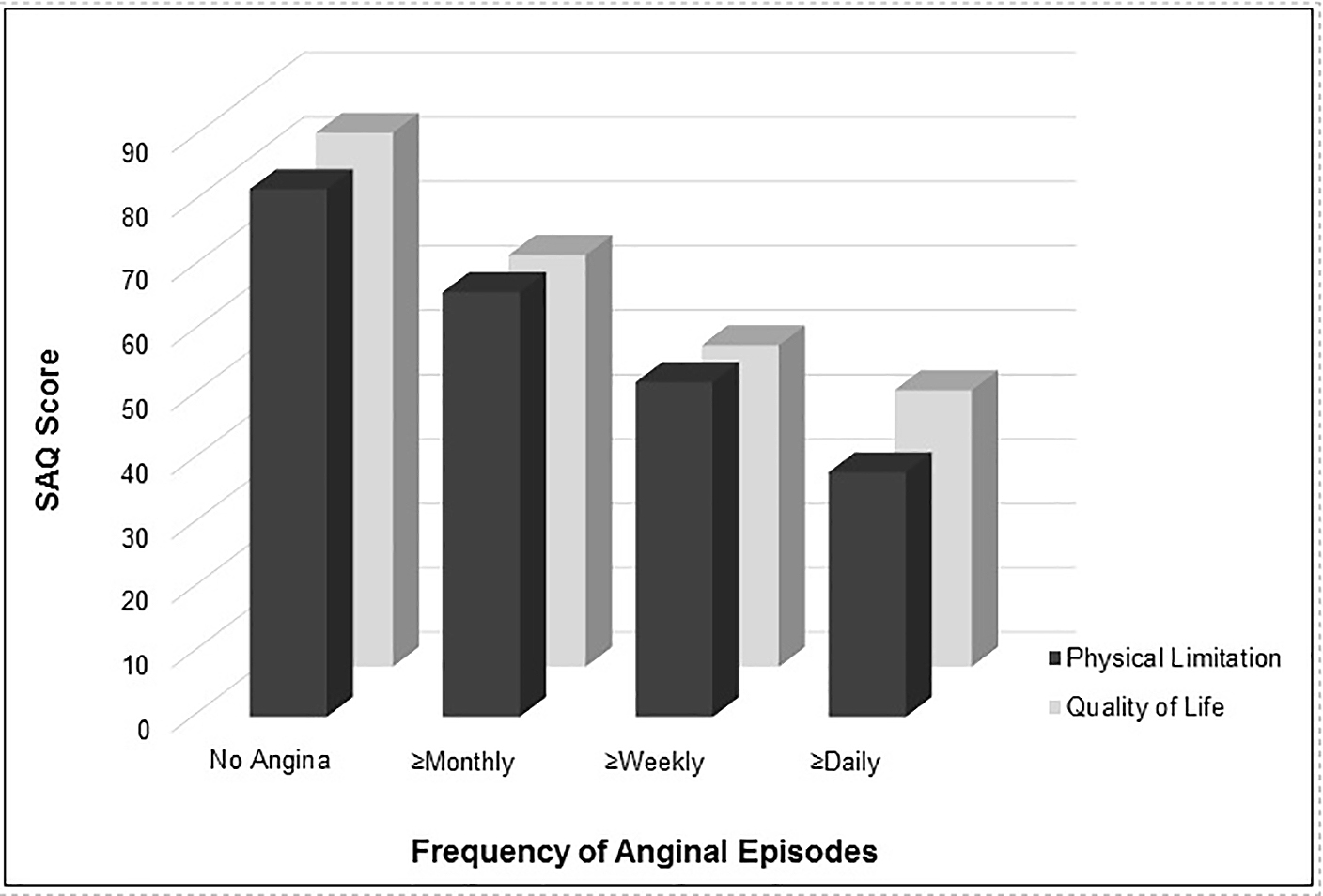
SAQ (Seattle Angina Questionnaire) scores obtained from stable angina patients attending primary care practice in Australia, higher score indicates better functioning.
Figure adapted with permission from Beltrame et al [20]
Optimising health status
The conventional treatment approach for patients with angina includes the prevention of cardiac events and the improvement in symptoms, although the later should be extended to the more holistic approach of optimising health status. These objectives can be achieved with medical therapy, rehabilitation and support services, and possibly revascularisation procedures, including percutaneous coronary intervention (PCI) and coronary artery bypass grafting (CABG). The role of these specific therapies varies with the clinical context since acute coronary syndromes are associated with a high risk of further cardiac events in the following 30 days, whereas chronic coronary syndromes have a comparative low risk of cardiac events. Accordingly, in acute coronary syndromes, medical and revascularisation therapies have a key role in preventing further cardiac events whereas the management of chronic coronary syndromes should particularly focus on the optimisation of health status. This later principle is exemplified by the COURAGE trial, which enrolled patients with chronic stable angina, many of whom had multivessel obstructive CAD. The patients were randomised to medical or revascularisation therapy, with no difference observed in cardiovascular events between these two treatment approaches. Moreover, PCI had only a small incremental benefit in reducing angina symptoms over optimal medical therapy alone. Accordingly, guidelines [22] and appropriateness use criteria [23] for chronic stable angina recommend utilising optimal medical therapy before consideration of revascularisation therapies.
The management of patients with angina has not only evolved to the holistic consideration of health status but also to evaluation of clinical performance criteria. Hence, CAD patients should routinely be prescribed antiplatelet agents, statins and ACE-inhibitors. In addition, anti-anginal agents and, if necessary, revascularisation therapies, should be initiated to reduce angina frequency and optimise health status. Moreover, considering the risks and costs associated with PCI, its efficacy should be assessed utilising “post-PCI angina” as a key performance marker.
CONCLUSION
Over the past 200 years, angina pectoris has evolved from a diagnosis based upon history alone to the coronary arteries being imaged in vivo via angiography, thereby identifying the presence of CAD. With this advancement in clinical diagnosis, it has become apparent that many patients with angina do not have obstructive CAD so that functional coronary disorders must be considered. Furthermore, with the continuing evolution of personalised medicine, controlling angina symptoms will only partially achieve optimal health status, with measures to improve the patient’s physical limitations and quality of life having an equally important role. Hence, the nature of angina and its management will continue to evolve in the future.