

Introduction
Successful treatment of STEMI is often offset by the resultant bleeding events. There seems to be a linear association between bleeding and death in patients with STEMI, regardless of the success or failure of reperfusion therapy [1]. Blood transfusions in this setting are known to result in higher mortality [2]. Despite diverse definitions in clinical trials, bleeding is also known to increase the rates of recurrent MI and stroke, and results in a longer hospital stay [1]. Gastrointestinal and intracranial bleedings carry a worse prognosis. Therefore, caution must be exercised to prevent bleeding complications, although urgent reperfusion/antithrombotic strategies are life-saving in STEMI. In general, fibrinolysis causes 0.9-1% of intracranial bleeds and 4-13% of major non-cerebral bleeds (defined either as those requiring blood transfusion or as those that are life-threatening) [3]. On the other hand, primary percutaneous coronary intervention (PCI) resulted in infrequent major bleeds (1.6%) in a large, prospective study [4]. There is heterogeneity in the definition of bleeding, and commonly used classifications include TIMI, BARC, GUSTO, PLATO, GRACE, etc.
Assessing the risk
Important risk factors for bleeding have been identified in several clinical trials [1,5]. They are listed below:-
- Advanced age, >75 years
- Female sex
- Low body weight
- Obesity
- Hypertension
- Heart failure or shock
- Diabetes mellitus
- Prior history of GI bleeding
- Chronic kidney disease
- High white blood cell count
- Anaemia
- Chronic oral anticoagulation
- Sepsis
Hypertension poses the particular hazard of intracranial haemorrhage (ICH) with an incremental risk beginning at systolic pressure >160 to 170 mmHg. Low body weight, <70 kg in women and <80 kg in men, is also a risk factor for ICH [1].
Risk scores can be used to stratify patients presenting with STEMI prior to the initiation of treatment, especially reperfusion therapy. A specific risk score for STEMI patients to estimate the bleeding probability is still elusive. The CRUSADE bleeding score [6], developed in patients with non-STEMI, can be extended to STEMI patients [1]. It has been well validated in patients with STEMI treated both with fibrinolysis and primary PCI [7]. The CRUSADE score contains eight criteria with varying point values defining bleeding risk as follows:-
- very low risk (bleeding score ≤20, 3.1% risk of major bleeding)
- low risk (21-30, 5.5%)
- moderate risk (31-40, 8.5%)
- high risk (41-50, 11.9%)
- very high risk (>50, 19.5%).
Major bleeding defined as intracranial haemorrhage, retroperitoneal bleed, haematocrit drop ≥12%, any RBC transfusion when baseline haematocrit ≥28%, or any RBC transfusion when baseline haematocrit <28% with witnessed bleed.
Fibrinolysis in patients with bleeding risk
Fibrinolysis is better avoided in patients with a significant bleeding risk. The recommended absolute and relative contraindications to fibrinolysis [3] are given in Table 1. In case of absolute contraindications to fibrinolysis or high risk for bleeding events, primary PCI should be considered, even if it cannot be performed within the guideline-endorsed timelines [1]. In patients who are considered to be at moderate risk for bleeding events and in those with relative contraindications to fibrinolysis, primary PCI should be preferred because it is associated with lesser rates of significant bleeding [8]. The decision for fibrinolysis should be based on a careful evaluation of the risk and benefit, taking into account duration of symptoms, time delay to PCI, patients’ comorbidities and haemodynamics. If the patient presents early, within two hours of symptom onset with a large infarct and is deemed to have low bleeding risk, fibrinolysis can be given, provided first medical contact to balloon inflation is >90 minutes [3]. Fibrinolysis in the pre-hospital setting is not encouraged in the presence of any contraindication to fibrinolysis and patients must be transferred to a PCI-capable facility.
Tenecteplase (TNK) seems to be the right choice of fibrinolytic agent in this patient subset that does not undergo primary PCI. TNK can be administered in a single bolus with dose adjustments according to body weight. It is equivalent to accelerated tissue plasminogen activator (tPA) for efficacy and has a significantly lower rate of non-cerebral bleedings with a reduced need for blood transfusion [9]. The dose can be halved in patients older than 75 years to reduce the incidence of ICH [10]. An elevated international normalised ratio (INR) higher than 1.7 or a prothrombin time (PT) longer than 15 seconds due to anticoagulation is a contraindication to fibrinolysis. Post-fibrinolysis anticoagulation is recommended to be given for at least 48 hours, and should involve careful dosing and close monitoring. Net clinical benefit favours enoxaparin over unfractionated heparin (UFH), but bleeding is more common with the former. The dose of enoxaparin should be adjusted in patients over 75 years and in those with renal impairment. If UFH therapy is used, activated partial thromboplastin time (aPTT) values >70 seconds are associated with a higher likelihood of bleeding [3]. Fondaparinux usage is currently limited to patients treated with streptokinase but warrants dose adjustment in a few patient subsets, and adjunctive anticoagulation with UFH is required if PCI is needed for any reason. It is imperative to remember that currently only UFH has an effective antidote (protamine) if immediate reversal of action is required due to bleeding.
Table 1. Contraindications to fibrinolysis [3].
|
Absolute |
Relative |
|---|---|
|
Previous intracranial haemorrhage or stroke of unknown origin at any time |
Transient ischaemic attack in the preceding 6 months |
|
Ischaemic stroke in the preceding 6 months |
Oral anticoagulant therapy |
|
CNS damage or neoplasms or AV malformation |
Pregnancy or within one week postpartum |
|
Recent major trauma/surgery/head injury (within the preceding 3 weeks) |
Refractory hypertension (systolic pressure >180 mmHg and/or diastolic pressure >110 mmHg) |
|
GI bleeding within the past month |
Advanced liver disease |
|
Known bleeding disorder (excluding menses) |
Infective endocarditis |
|
Aortic dissection |
Active peptic ulcer |
|
Non-compressible punctures in the past 24 hrs (e.g., liver biopsy, lumbar puncture) |
Prolonged or traumatic resuscitation |
Primary PCI in patients with bleeding risk
Primary PCI should be the default procedure in patients with STEMI considered for reperfusion strategy if at significant risk for bleeding events. However, bleeding is more frequent when PCI is performed during STEMI compared to an elective procedure. The risk factors identified which increase the chances of haemorrhagic complications during primary PCI are:-
- Inappropriate dosing of antithrombotic drugs
- Femoral access
- Number of punctures
- Sheath size
- Late removal of sheath post procedure
- Prolonged duration of the procedure
- Intra-aortic balloon pump
- Use of GP IIa/IIIb inhibitors
- Low molecular weight heparin within 48 hours of PCI
The radial route is the preferred access route in primary PCI, especially in patients with any bleeding risk. Many studies have demonstrated its advantage, including the MATRIX study which showed the superiority of the transradial approach over the transfemoral in reducing net adverse clinical events and bleeding complications in 8,404 patients with acute coronary syndrome (ACS), 48% of whom were patients with STEMI [11]. The transradial access seems to be particularly important in reducing bleeding complications and mortality in female patients. If the femoral route is employed, fluoroscopy or an ultrasound-guided puncture may reduce access-related bleeding. The role of vascular closure devices in reducing bleeding is inconclusive.
Guidelines recommend dual antiplatelet therapy (DAPT) with aspirin and an adenosine diphosphate (ADP) receptor blocker along with a parenteral anticoagulant in patients undergoing primary PCI [3]. A lower permissible dose of antiplatelets should be used if the risk of bleeding outweighs the benefits. Patients can be preloaded with aspirin and clopidogrel. Aspirin 150 mg loading followed by 75 mg daily [12] is preferred, based on studies comparing higher- with lower-dose aspirin. Aspirin significantly increases recurrent haemorrhage in patients with bleeding peptic ulcer but decreases mortality [13]. A loading dose of clopidogrel of only 300 mg is recommended for clopidogrel-naive patients at risk of bleeding (who undergo PCI within 24 hours of fibrinolysis) [1]. The benefits of prasugrel or ticagrelor compared to clopidogrel must be weighed against the risk of bleeding. Prasugrel is contraindicated in patients over 75 years old, with prior stroke or TIA and low body weight (<60 kg). Proton pump inhibitors (PPI) are appropriate in patients with risk factors for GI bleeding.
A recent meta-analysis which included 17,294 patients from six major randomised trials showed that bivalirudin reduced major bleeding and death compared with conventional antithrombotic therapy in patients undergoing primary PCI [14]. The increases in the rate of acute stent thrombosis were neutralised by prolonging the bivalirudin infusion for three hours after the procedure with no further excess in bleeding events. Enoxaparin has no benefit over UFH in reducing bleeding events and dose adjustments should be made to balance ischaemia and bleeding. Again, an effective and total antidote is available only for UFH, if required for severe bleeding. Routine use of GP IIb/IIIa inhibitors is not encouraged in patients with contraindications [3]. If bail-out therapy is considered, abciximab is the best choice as it has a lower risk of bleeding and the most data among GP IIb/IIIa inhibitors. Moreover, the effect of the drug can be reversed by platelet transfusions in case of active bleeding. Routine anticoagulant therapy is not indicated after primary PCI [3].
Bare metal stents (BMS) are preferable to drug-eluting stents (DES) in patients at risk for bleeding, unless the latter are absolutely indicated [1]. The recently published NORSTENT trial has demonstrated comparable outcomes of death and non-fatal MI at five years between patients who received second-generation DES or BMS [15]. Balloon angioplasty alone without stent placement can also be considered in these patients [1]. The novel polymer-free DES BioFreedom™ (Biosensors International, Singapore) has demonstrated better outcomes in patients with high bleeding risk when compared to BMS at 390 days with only one month of DAPT [16].
Primary PCI should be performed through the radial route in patients on therapeutic oral anticoagulation with appropriate additional antithrombotic drugs as required, regardless of the last dose of oral anticoagulant [1]. Bivalirudin is preferred because of its lower bleeding risk, especially when dabigatran is the oral anticoagulant [12]. Enoxaparin is favoured in case of direct anti-Xa inhibitors (rivaroxaban or apixaban) to avoid crossover [12]. GP IIb/IIIa inhibitors are reserved only for bail-out situations [12]. Parenteral anticoagulants should be stopped immediately after primary PCI [12]. In a small retrospective study of patients on chronic anticoagulation with INR in the therapeutic range, PCI did not result in excessive bleeding when additional periprocedural anticoagulation was not given [17], but this study included only a small percentage of ACS patients.
Conservative management
Currently, there is no consensus on the role of PCI in patients presenting >12 hours of symptom onset in the absence of evidence of ongoing ischaemia [3]. Especially in patients with bleeding risk, an invasive strategy can be avoided if the patient presents late in STEMI with stable haemodynamics and no evidence of ischaemia. In clinically stable patients with a small infarct area and high bleeding threat, the risk/benefit of conservative management vs. an invasive strategy should be considered and treatment should be tailored accordingly.
Coronary bypass graft surgery (CABG)
The role of CABG in the acute phase of STEMI is small, and there are no data/recommendations to support it in patients with bleeding risk.
Conclusion
Patients with STEMI at risk for bleeding constitute a unique and difficult subset to treat. At present, there is a dearth of clear recommendations to guide management strategies. The objective in these patients is to minimise the risk of bleeding while successfully treating thrombotic/ischaemic complications. Randomised studies focused on finding this balance are needed in the STEMI population. An individualised treatment weighing the risk and benefit could be more appropriate when selecting agents from the currently available armamentarium.
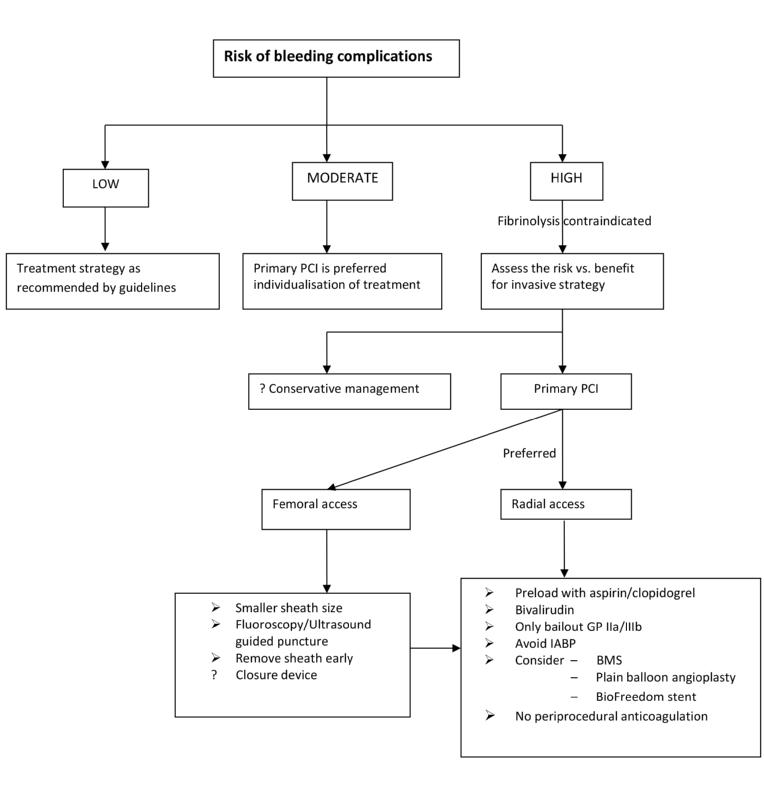
Figure 1. Prevention of bleeding in STEMI patients.