Barcelona, Spain – Sunday 31 August 2014: Renal denervation seems to be more successful at reducing blood pressure in patients with resistant hypertension when it includes accessory renal arteries, according to research presented at ESC Congress today by Dr Linda Schmiedel from Germany.
Dr Schmiedel said: “More than one billion people worldwide suffer from arterial hypertension, which is defined as blood pressure (BP) greater than 140/90 mmHg. Up to 15% of patients suffer from resistant hypertension (rHTN) and are unable to reduce BP below 140/90 mmHg despite adhering to full doses of an appropriate three drug treatment regimen including diuretics.” (1)
She added: “The prevalence and prognosis of rHTN is still unknown, but we do know that cardiovascular risk doubles with each BP increment of 20/10 mmHg. Effective BP treatment is therefore vital, especially in patients with rHTN.” (2)
Renal sympathetic denervation (RDN) has been established as an effective treatment for these patients since 2009. It works by decreasing renal sympathetic nerve activity using point-by-point radiofrequency application in the main renal arteries. The procedure is feasible in these arteries because of their size (>20mm long and 4mm in diameter). RDN has shown promising results with BP reductions of 23/11 mmHg in previous studies (3).
But until now, RDN has not been performed in the accessory renal arteries due to their small diameter and the risk of developing a vascular stenosis after catheter ablation.
The aim of the current study was to examine whether complete ablation by performing RDN in accessory renal arteries, in addition to the main renal arteries, would influence blood pressure even more in patients with rHTN. The study included 110 patients with rHTN. At the beginning of the study, mean ambulatory BP was 154±10/85±9 mmHg and patients were taking more than 6 drugs to treat their hypertension.
Six months after RDN, 62 patients were available for follow up and had office BP (OBP) and 24 hour ambulatory BP (ABPM) measurements taken. Overall, the procedure was successful in 42 patients (67%) with a corresponding drop in BP of more than 10 mmHg (figure 1). Of these patients, 34 (54.8%) had complete ablation including the main and accessory arteries.
Dr Schmiedel said: “Our results show that more than half of patients with successful RDN had complete ablation including the main and accessory arteries. Complete ablation seems to be an important factor in achieving success with this procedure.”
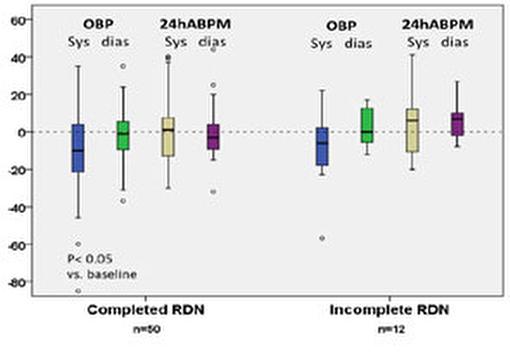
Out of the 62 patients available at follow up, 12 (19%) had accessory renal arteries that were not completely ablated. The success of RDN was compared between those whose ablation was complete (including main and accessory arteries) compared to those whose ablation was incomplete (main arteries only). Patients with complete ablation had a greater BP reduction with RDN (18±4/-5±2 mmHg) compared to those whose ablation was incomplete (12±8/3±4 mmHg) but the difference was not significant (p=0.67) (figure 2).
Dr Schmiedel said: “We found that complete ablation produced a noticeable trend for more BP reduction although it was not significant, maybe due to the limited amount of patients. Taking our results together we can conclude that RDN is an effective procedure for treating resistant hypertension but success depends on careful selection and completeness of ablation.”
She concluded: “Further investigations focused on the role of accessory renal arteries and the completeness of the RDN procedure are needed to confirm our results.”