Paris, France – Aug. 30, 2011: Since 2007 Transcatheter Aortic Valve Implantation (TAVI) has become an alternative treatment for elderly patients with severe aortic stenosis at high risk for surgical aortic valve replacement. At present, durability and hemodynamic performance of transcatheter aortic valves remain unclear. Our single center data of the German Heart Center in Munich demonstrates a sustained improvement of hemodynamic performance up to 3 years after CoreValve implantation.
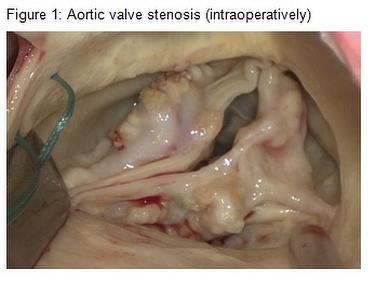 Aortic valve stenosis (AS) is the most frequent heart valve disease in Europe and North America. The most common type is a chronic progressive calcific stenosis, the incidence increases with age. Echocardiography is the main diagnostic tool to assess presence and severity of AS. Severe calcification of the aortic valve can be found in 13% of the population >75 years; at least moderate AS can be found in 5% (Lindroos et al. JACC 1993, 21:1220-1225). Due to demographic developments, an increase of aortic valve stenosis is expected for the next decades.
Aortic valve stenosis (AS) is the most frequent heart valve disease in Europe and North America. The most common type is a chronic progressive calcific stenosis, the incidence increases with age. Echocardiography is the main diagnostic tool to assess presence and severity of AS. Severe calcification of the aortic valve can be found in 13% of the population >75 years; at least moderate AS can be found in 5% (Lindroos et al. JACC 1993, 21:1220-1225). Due to demographic developments, an increase of aortic valve stenosis is expected for the next decades.
If severe AS becomes symptomatic, the prognosis is poor without therapy and average survival is < 2-3 years (Bonow et al. Circulation 1998, 98:1949-1984). The therapy of choice is a surgical aortic valve replacement. Without serious comorbidities, the operative mortality is low (1-3%). Operative mortality increases with the age of the patients (octogenarians 4.9%, nonagenarians 9.6%) and prevalent comorbidities (up to 25%) (Brown et al, J Thorac Cardiovasc Surg, 2009;137:82-90). However, up to 30% of patients with severe symptomatic AS do not undergo surgery because of their high surgical risk. For these patients a less invasive therapy would be a good alternative.
Transcatheter aortic valve implantation (TAVI) was introduced in 2002 by Alain Cribier (Cribier et al. Circulation 2002, 106:3006-3008). The current technique is to crimp a bioprosthetic valve on a catheter, inserting the catheter through a peripheral artery or the apex of the heart and implanting the valve within the calcified native aortic valve. After developing different valve types and techniques, achieving a high rate of successful implantations (99%) and increased safety of the procedure during the last years, TAVI developed an alternative treatment for elderly patients with severe aortic stenosis at high risk for surgical aortic valve replacement. Until the end of 2010 approximately 30 000 transcatheter aortic valves were implanted worldwide.
Biological aortic valve prostheses have been implanted and examined for almost 50 years. Their durability is limited to 10-15 years, due to degeneration of the prosthetic valve material (porcine, bovine or human). Whether durability and hemodynamic performance of transcatheter aortic valves are comparable to conventional biological aortic valve prostheses remains unclear. The first data after 3 years of TAVI are now available.
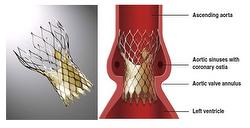
TAVI procedures have been performed at the Department of Cardiovascular Surgery of German Heart Center Munich since June 2007. We studied 393 consecutive patient implants with the CoreValve prosthesis1 from June 2007 to June 2011. The CoreValve prosthesis consists of a self expandable nitinol stent with a porcine pericardium valve. So far, there a two sizes available: 26mm and 29mm.
Figure 2: CoreValve 1 Prosthesis
To study hemodynamic valve performance, transthoracic echocardiography was performed preoperatively, at discharge and at 6, 12, 24 and 36 months.
We collected the following data: transaortic valve mean and peak gradient (Pmean, Pmax, severity of the stenosis raises with gradients), effective orifice area (EOA) using continuity equation (calculates the area of the open valve in cm²), enddiastolic septal wall thickness (wall of the left ventricle is usually hypertrophic with artic valve stenosis), left ventricular ejection fraction (LVEF) and severity and origin of aortic regurgitation (central/paravalvular).
393 patients (220 female, 173 male) with a mean age of 80 years (+/-7) underwent implantation with a CoreValve device. Due to anatomical conditions, a 26 mm prosthesis was implanted in 37% and a 29 mm prosthesis in 63% of the patients. A transfemoral approach was possible in 87% of the patients, 11% of the CoreValves were implanted via subclavian artery, 1% transapical, 1% via ascending aorta.
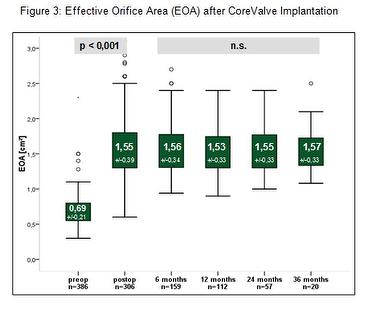
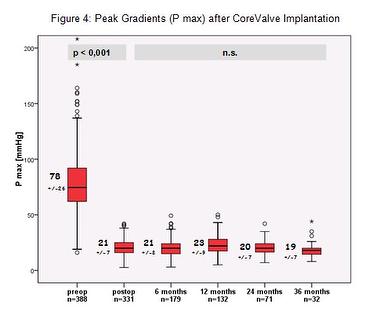
EOA increased significantly after TAVI (p<0,0001). Peak and mean aortic valve gradients decreased significantly after TAVI (p<0,0001). At 6, 12, 24 and 36 months we did not find any observable change in EOA, P mean and P max. End diastolic septal wall thickness was reduced significantly at 12 and 24 months, compared to baseline (preoperatively 14.9+/-2 mm, 24 months 13.8+/-1 mm (p<0,001). There was evidence of improvement of the LVEF 12 months after TAVI. In the setting of heavy calcification of the aortic valve paravalvular aortic regurgitation (AR) is a common finding following CoreValve implantation. In our group 64% of the patients had AR (trivial or mild 65%, mild to moderate 20%, moderate 15%). Origin of the regurgitation was in 95% paravalvular.
Contributors:
Opitz A. (MD),
Hettich I., Hutter A., Bleiziffer S., Ruge H., Piazza N., Mazzitelli D., Lange, R.
1 Medtronic.
Conclusion:
Our single centre data of the German Heart Centre Munich demonstrate a sustained improvement of hemodynamic values up to 3 years after CoreValve implantation. There are no signs of unexpected early degeneration of the CoreValve prostheses. Further monitoring of the patient group will be published.