
The case
Description
- A male amateur athlete (56 years, BMI 22.8 kg/m2) suffered a transient ischemic attack during a mountain race.
- He now complained of a reduced exercise capacity after a period of no exercise training.
- Prior to the event, the patient exercised 5 times per week for 1 to 2 hours per session, cross-country skiing during winter and running and cycling during summer, and participated in official competitions.
- He had a history of arterial hypertension which was treated with an ACE-Inhibitor.
- Family history was negative for cardiovascular disease.
- The electrocardiogram showed a normal sinus rhythm, 65 beats per min, without depolarisation or repolarisation abnormalities.
- A transthoracic echocardiography showed concentric left ventricular remodeling with normal systolic function and first degree diastolic dysfunction, mildly dilated atria, without relevant valvular dysfunction nor pulmonary hypertension.
- Transoesophageal echocardiography revealed neither thrombi nor persistent foramen ovale.
- Seven days Holter monitoring revealed no atrial fibrillation.
A cardiopulmonary exercise test was performed for the following questions:
- Determination of exercise capacity.
- Blood pressure response during exercise.
- Heart rate kinetics and exercise-related arrhythmias.
- Exercise-related pulmonary hypertension (ventilation-perfusion mismatch)
- Determination of training zones based on ventilator thresholds to guide re-uptake of exercise training.
Test findings
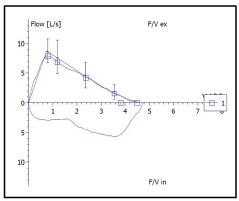
- The resting spirometry showed a FVC of 4.5 l (99% predicted), a FEV1 of 3.8 l (106% predicted), and a FEV1/FVC of 85%. Estimated maximum voluntary ventilation (MVV, FEV1*40) was 152 l.
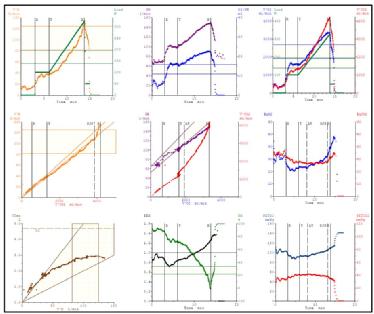
- A standard ramp protocol for athletic individuals was chosen. The test started with 3 min rest (R), followed by 3 min constant load at 100 watt, followed by a ramp (30 watt/min) (T) until exhaustion, ending with a 4 min recovery period at 50 watt (R) (Panel 3).
- Exercise capacity was above average with 316 Watt (4.3 Watt/kg, 189 % predicted), and a peak VO2 of 45.8 ml/min/kg (13.1 MET, 146 % predicted) (Panel 3).
- Blood pressure increased from 130/75 mmHg to 200/95 mmHg at peak exercise.
- Heart rate increased from 79 beats per min to 148 beats per min (90% predicted).
- Heart rate recovery in the first min after exercise was 22 beats (Panel 2).
- No arrhythmias or ST depressions occurred.
- Maximum rate pressure product was 29600 mmHg/min.
- Maximum respiratory exchange ratio was 1.22 (Panel 8).
- The patient was exhausted at the end of the test (Borg 19/20).
- Maximum ventilation was 135 l (Panel 1)
- Breathing reserve ((1-VEmax/MVV)*100) was 11% (Panel 8).
- Respiratory efficiency, determined by the VE/VCO2 slope was 25 (Panel 4).
- Peak PETCO2 was 42 mmHg (Panel 9).
- The O2 pulse (VO2/heart rate) increased to 22.6 ml (170% of predicted, Panel 2).
- The VO2/work rate slope was 8.8 ml/min/watt (Panel 3).
- The first ventilatory threshold (anaerobic threshold, AT) could be determined in Panel 6 (increase in EqO2) and Panel 9 (increase in PETO2), but not in Panel 5.
- The second ventilatory threshold (respiratory compensation point, RCP) could be determined in Panel 6 (increase in EqCO2), and Panel 9 (decrease in PETCO2), and could be confirmed in Panel 4 (increase in VE/VCO2 slope).
Spirometry
9 Panel Plot of the Cardiopulmonary Exercise Test
Test your knowledge
Interested in learning more?
Access the ESC e-learning platform on prevention, cardiovascular risk factors and sports cardiology .
Not yet an EAPC member ?
Note: The views and opinions expressed on this page are those of the author and may not be accepted by others. While every attempt is made to keep the information up to date, there is always going to be a lag in updating information. The reader is encouraged to read this in conjunction with appropriate ESC Guidelines. The material on this page is for educational purposes and is not for use as a definitive management strategy in the care of patients. Quiz material in the site are only examples and do not guarantee outcomes from formal examinations.