
The case
Description
- This male patient (66 years, BMI 25 kg/m2, current smoker) has a history of bilateral pulmonary embolism in June 2013 which was treated with EKOS-lysis (ultrasound-enhanced thrombolysis). He is currently under oral anticoagulation.
- During work-up, coronary artery disease (CAD) with a high-degree right coronary artery stenosis was detected. A percutaneous coronary intervention (PCI) was performed in July 2013. Left ventricular ejection fraction was slightly reduced (50%).
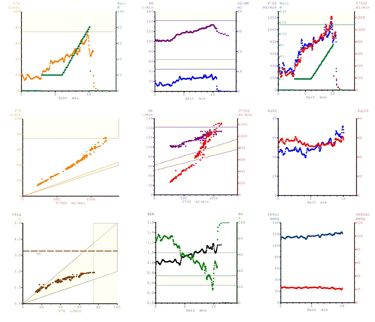
- This is the cardiopulmonary exercise testing (CPX) 9 panel plot at the beginning of a 3-month ambulatory cardiac rehabilitation program. The patient complained of persisting exertional dyspnoe NYHA III, but no chest pain, dizziness or syncope.
- Pulmonary function test (PFT) was performed: Forced Vital Capacity (FVC): 3.0 L (71% predicted); Forced Expiratory Volume in 1 second (FEV1): 2.6 L (79% predicted). FEV1/FVC ratio 85%.
Test findings
- The 9-plot analysis documented a reduced exercise capacity with 81 Watt (51% predicted), and a peak VO2 of 1130 ml/min, 14.0 ml/min/kg (55% predicted) (Panel 3).
- The O2 pulse (VO2/heart rate) (Panel 2) and the VO2/work rate slope (Panel 3) were reduced.
- The VE/VCO2 slope was markedly elevated with a value of 50 (Panel 4).
- Breathing reserve (1- ratio of ventilation at maximal exercise to maximal voluntary ventilation) was 0.18 (Panel 8).
- PETCO2 was low at rest (23 mmHg) and did not increase during exercise (Panel 9).
- Blood pressure was 115/70 mmHg at rest and 120/80 mmHg at maximum exercise. SpO2 was not recorded due to a technical problem. Exercise ECG revealed no exercise-induced ischemia.
Test your knowledge
Interested in learning more?
Access the ESC e-learning platform on prevention, cardiovascular risk factors and sports cardiology .
Not yet an EAPC member?
Note: The views and opinions expressed on this page are those of the author and may not be accepted by others. While every attempt is made to keep the information up to date, there is always going to be a lag in updating information. The reader is encouraged to read this in conjunction with appropriate ESC Guidelines. The material on this page is for educational purposes and is not for use as a definitive management strategy in the care of patients. Quiz material in the site are only examples and do not guarantee outcomes from formal examinations.