
The study and diagnosis of acute myocarditis is complicated by all of its clinical expressions, from subclinical ventricular arrhythmias to severe heart failure requiring cardiac transplantation. Many myocarditises are not clinically obvious and some symptoms may not be appropriately interpreted, thus the true incidence of myocarditis is not known - estimated at 1 to 10 cases per 100,000 persons each year. While studies have attributed myocarditis to 1% to 1.5% of the sudden and unexpected deaths (1), the incidence of sudden death among patients with myocarditis however, is not well documented.
Just as myocarditis can take on many forms, a wide variety of situations can trigger it (2, 3). Viral infections represent the most common aetiology in western countries. Viruses usually encountered are adenovirus, parvovirus B19, human herpesvirus 6 and enterovirus (4). Less often, myocarditis can be due to sarcoidosis, Crohn’s disease, toxins, drug reactions, or various other infectious agents. Although cardiotropic viruses infect more than 90% of the general population, it is estimated that only 1% to 5% of infected patients will develop histologically-proven myocarditis (5).
Regarding sudden death within the context of myocarditis specifically, several viruses have been associated with increased risk. One study revealed adenovirus serotype 5 as responsible for fatal cases of acute myocarditis in Cuba (6, 7). Coxsackievirus B3 infection may also be associated with increased risk of arrhythmias owing to increased intracellular calcium and decreased magnesium levels in cardiomyocytes (8).
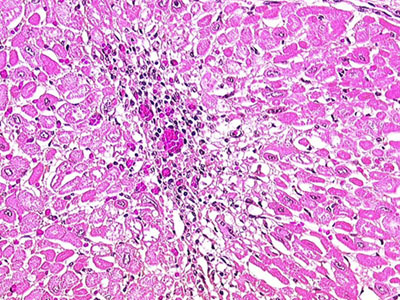
Fig. 1 : Myocardial biopsy: Lymphocyte-rich inflammatory infiltrate associated with myocyte degeneration (Hôpital Louis Pradel, Lyon, France).
1 - Relationship between myocarditis and ventricular arrhythmia
Given that we are all exposed to cardiotropic viruses and fewer than 10% of subjects who are infected develop histologically-confirmed myocarditis, genetic predispositions may come in to play (5). The autoimmune response appears to be the major contributing factor to cellular injury during viral infection, which, in turn, may trigger ventricular arrhythmia. Experimental data has shown that the autoimmune component of myocarditis is mainly controlled by non-MHC (major histocompatibility complex) genes, and that MHC class II genes modify the severity of the disease (9).
In parallel, an association between acute myocarditis, ventricular arrhythmias and various myocardial channelopathies has been suggested (10, 11, 12). A recent study using the whole genome approach has identified a higher incidence of a polymorphism next to the CXADR gene when compared to a control group without sudden death (13). This gene codes for a viral receptor implicated in dilated cardiomyopathy and has recently been identified as a modulator of the cardiac electrical conduction system.
Our group previously, had reported ECG abnormalities consistent with three types of channelopathies - Brugada syndrome, short QT syndrome and early repolarisation - in three patients with acute myocarditis complicated by ventricular fibrillation (10). In the two patients who survived the acute phase, ECG findings persisted to suggest that these abnormalities were not due to the myocarditis itself. Other observations have shown an association between Brugada syndrome, myocarditis and sudden death (11, 12). Temperature-dependent modifications of cardiac ion channel properties could also be involved (14). The Brugada electrocardiographic pattern appears to be more pronounced during a febrile state (15, 16). Frustaci et al. (12) concluded that up to 77% of patients with a clinical phenotype of Brugada syndrome and sustained ventricular arrhythmias could actually have an acute myocarditis which could mimic the electrocardiographic pattern of Brugada syndrome. It may be speculated that unknown ionic channel dysfunction could become clinically obvious during an infectious insult.
Various hypotheses have been put forward to explain the occurrence of episodes of ventricular arrhythmia during acute myocarditis. Viral-induced myocardial fibrosis and secondary hypertrophy could favour a regional slowing of action potentials, which could result in re-entry circuits. Ventricular arrhythmia could also be triggered by small, focal inflammation in electrically sensitive myocardial areas. As stated above, myocardial ischemia could also be implicated as well as abnormal function of myocardial ion channels.
2 - Diagnosis, treatment and prognosis
During episodes of acute myocarditis with ventricular arrhythmia, Troponin T and I are more useful when a high sensitivity threshold is used. Depending on the extent of myocardial damage, electrocardiographic abnormalities range from T wave inversion to frank ST-elevation with bundle branch block. Magnetic Resonance Imaging (MRI) enables the visualisation of the entire myocardium and is thus well suited to detect the focal patchy nature of the myocardial lesions. Endomyocardial biopsy is not necessary for the diagnosis of myocarditis.
Immunosuppression, interferon, intravenous immune globulin and immune adsorption therapy are sometimes used to treat myocardial inflammation, but strong evidence of the benefit of these therapies is lacking. Targeted vaccination against the most common causative agents may be developed in the future.
It is difficult to establish the exact prognosis of patients with ventricular arrhythmias complicating acute myocarditis. There are few long-term studies dealing with this issue. It is suggested that the prognosis of patients with resuscitated sudden cardiac death in the onset of acute myocarditis is favourable, arrhythmias usually being self-limited with no recurrences that follow the acute phase (17, 18).
Conclusion:
The mechanisms underlying the occurrence of ventricular arrhythmias during myocardial inflammation are unknown. The extent of cellular damage that follows acute myocarditis could be genetically determined and likewise, the presence of severe arrhythmias during the onset of acute myocarditis could reveal pre-existing cardiac channelopathies. Therefore, it is recommended to look for an arrhythmogenic substrate in patients with ventricular fibrillation triggered by acute myocarditis. Additionally, MRI should be performed in patients resuscitated from sudden cardiac death, to rule out myocardial inflammation.
With the help of molecular biology, it is likely that we will increase our understanding of electrical instability in the context of myocarditis. Enhanced identification of patients at risk of sudden death during myocardial inflammation will hopefully be the first clinical application to ensue.