
TAVI is a therapeutic alternative when aortic valve replacement (AVR) is contraindicated for reasons of 1) technical complexities or 2) severe comorbidities amounting to high surgical risk. TAVI is performed either 1) via an antegrade transapical approach through the apex of the left ventricle by anterolateral thoracotomy or 2) by retrograde approach through vascular access, most oftentimes the common femoral artery.
Complications of the antegrade transapical approach
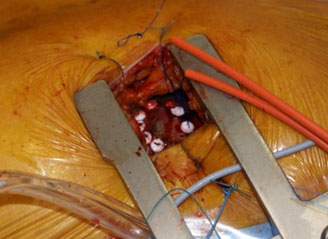
TAVI is performed through a left antero-lateral mini-thoracotomy under general anaesthesia, with fluoroscopic and TEE guidance. A sheath is inserted into the femoral artery to perform angiography and allow immediate cannulation of the femoral artery for establishment of cardiopulmonary bypass. The pericardium is opened and suspended to the thoracic wall and the left ventricular apex is punctured through 2 purse-string sutures reinforced by Teflon pledgets (figure 1).
Figure 1. The antegrade transapical approach to aortic valve implantation.
The valve is crimped just prior to implantation and introduced through a sheath placed in the left ventricle in an antegrade fashion. It is positioned within the aortic annulus, and then delivered by balloon inflation under rapid ventricular pacing (1,2).
A) Postoperative mortality
The Edwards SAPIEN Aortic Bioprosthesis European Outcome (SOURCE) Registry provided 30-day outcome data for the TF approach in 463 patients. Total 30-day mortality was 6.3%, while it was 10.3% in the TA group (575 patients). Logistic EuroSCORE >30% and missing ejection fraction were found to be the only independent predictors for 30-day mortality (3).
Freedom from death at 30 days in all Edwards SAPIEN® THV Studies for the transfemoral approach was 91.8%, 92.7%, 86.7% and 93.7% for the PARTNER EU, REVIVAL, REVIVE, SOURCE studies, respectively and likewise in the TA group, freedom from death was 81.2%, 82.5% 84.7% and 89.7% respectively.
In a study conducted within our own practices, 50 patients with a mean age of 83±6 years were treated with TAVI, and a predicted surgical mortality of 28±14% and 16±7% using the EuroSCORE and STS-PROM, respectively. Thirty- five patients were treated via the TF, and 15 via the TA approach using the Edwards SAPIEN valve. Patients in the TA group had a greater number of comorbidities and consequently, a more critical early postoperative period and lower overall survival (4). Analysis of the mortality patterns revealed that per-procedure death only occurred in the transfemoral group. On the other hand, post-procedure in-hospital death was greater in the TA group adding as well in this group of patients to a higher risk since they had more severe peripheral artery disease, more frequent coronary artery disease, previous coronary artery surgery and myocardial infarction, renal failure, and extracardiac comorbidities, all known to negatively affect survival (5,6). In general, hospital mortality was mostly due to cardiac causes whereas once the patient passed the critical postoperative period, mortality was due to non-cardiac causes in half the patients (7).
B) Positioning and deployment
Immediate procedural success in the SOURCE registry was 92.7%. Other single-institutional studies reported a 100% success rate (8,9). A multicenter study reported successful positioning in 55 patients (93%) with the remaining four patients requiring conversion to sternotomy, as the valves were incorrectly positioned (10). Malposition of the valve, defined as either a too high or too low a deployment leading to aortic regurgitation or coronary obstruction was reported in 1.4% of cases in the SOURCE registry and all required a valve-in-valve procedure. In a study from Dallas and Cleveland, 88% of valves were successfully seated. Valve embolisation was observed in 5% and required open aortic valve replacement (11). The overall incidence of valve embolisation in the SOURCE registry was 0.5%. Conversion to open heart surgery and postoperative aortic replacement>grade 2+ were significant risk factors for 30-day mortality (table 1) (3).
C) Aortic insufficiency
Temporary intravalvular regurgitation during the procedure is commonly observed due to pressure of the stiff guidewire onto the cusps thus inducing valve incompetence. Removal of the guidewire resolves the problem (12). More enduring leaks have been described in several registries regardless of the type of prosthesis or approach for TAVI. In the FRANCE registry, 9.5% of all patients implanted with either the Sapien transcatheter valve or the CoreValve bioprosthesis (Medtronic) had grade 2 or more paravalvular leaks (13). The management of severe AR observed immediately following implantation consists of balloon re-dilation, and if this strategy is ineffective, implantation of a second valve in the valve is in order. In the SOURCE Registry AR >grade 2+ was observed in 13 patients (2.3%) of which 11 had a valve-in-valve treatment (3). The Multicenter Canadian Experience reported the need for second valve implantation in 9 procedures out of a total of 345 (2.6%) because of valve embolisation, valve malposition, and/or severe postimplatation regurgitation (14). When the leak is associated with severe hemodynamic disturbances, circulatory support can be provided in the form of a heart-lung or ECMO machine (15).
Table 1. Mortality rate with and without conversion to AVR and AR>2+ in Transapical TAVI Patients.
|
Risk Factor (RF) |
Mortality without RF |
Mortality with RF | P-Value |
|---|---|---|---|
| Conversion to AVR | 9.0% | 45.0% | <0.0001 |
| AR >2+ post procedure | 9.1% | 53.9% | <0.0001 |
D) Acute mitral insufficiency
We observed severe mitral regurgitation (MR) immediately after introduction of the guide wire into the left ventricular cavity due to entanglement of the guide wire with the mitral valve chordae. Traction on the subvalvular apparatus by the guide wire induced acute MR and lead to cardiovascular collapse. Retraction and repositioning of the guide wire through a different angle avoiding the mitral chordae was sufficient to establish mitral competence and hemodynamic stability.
E) Cardiac arrhythmias and heart block
Major ventricular tachyarrhythmia have been reported in 0% to 4% of TAVI patients and supraventricular tachyarrhythmia in 5%–31% of these. On the other hand, bradyarrhythmia requiring permanent pacemaker insertion were described in 0% to 36% (16) of these. Atrioventricular block occurs from the pressure applied on the conducting tissues located in the LV outflow tract and interventricular septum. Potential risk factors also include aggressive oversizing and the presence of pre-existing infranodal conduction anomalies such as right bundle branch block or second-degree heart block (17). The incidence of permanent pacemaker implantation was 7.3% in the SOURCE registry (4). Continuous post-operative ECG monitoring should be performed for at least 3 days in all patients, and until discharge in patients with increased risk for this complication (18).
F) Vascular complications
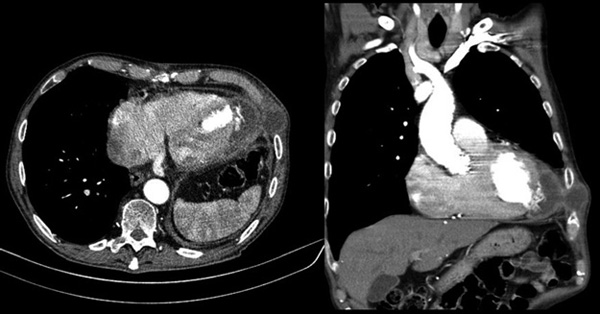
Femoral arterial puncture is required to perform aortography and provides a safety net for immediate insertion of cannula should the need for extracorporeal circulation arise. Seven major vascular complications involved 2.4% patients in the SOURCE registry and consisted of aortic dissections, aortic annular rupture and complications of the left ventricular apex. Patients with major vascular/access complications showed a high mortality rate with 50% of patients dying after surgery, which was significantly higher than the mortality rate observed in patients who did not experience major vascular/access complications (p < 0.001) (4). A case of false aneurysm of the left ventricular apex was observed 3 months after transapical TAVI using an introducing sheath of 33Fr (figure 2) (19).
Figure 2 : A case of false aneurysm of the left ventricular apex was observed 3 months after transapical TAVI using an introducing sheath of 33Fr.
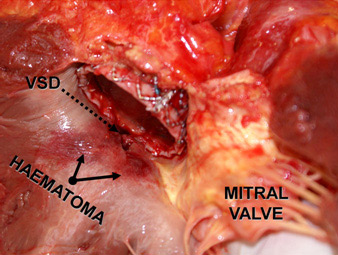
This list of complications with TAVI is not exhaustive. Other complications such as coronary artery occlusion, myocardial infarction, ventricular septal defect (figure 3), cardiac tamponade, rupture of the aortic annulus, renal failure etc. have been observed (12, 20, 21).
Figure 3. A case of ventricular septal defect.
Conclusion:
TAVI being new, implies learning from experience but also from mistakes. Several factors contribute to reducing the incidence of these complications: progress in imaging by echocardiography and quality fluoroscopy is of significant importance, improved intra-operative techniques and future smaller devices and lastly, the learning curve and experience in the optimal selection of patients should improve outcomes of TAVI.