Key points
- Insulin resistance (IR) is the most accepted unifying theory to explain the pathophysiology of the MS, which is nowadays the most prevalent risk factor for atherothrombotic disease.
- Current methods to quantify IR are cumbersome and only needed in clinical trials and for investigative purposes.
- In the clinical scenario, the TG/HDL ratio has been proved to have a high correlation with prevalence of MS and with IR.
The definition and clinical significance of metabolic syndrome
Metabolic syndrome (MS) is a cluster of risk factors for cardiovascular disease and type 2 diabetes mellitus (DM2) which occur together more often than by chance alone.
These risk factors include:
a) raised blood pressure;
b) a distinct dyslipidemic phenotype (raised triglycerides and lowered high-density lipoprotein cholesterol);
c) altered glucose metabolism;
d) central obesity. The different diagnostic criteria been proposed by different organizations over the past decade are summarized in table 11,2.
Table 1. The four main definitions of metabolic syndrome
| WHO (1998) | EGIR (1999) | ATP (2005) | IDF (2005) |
|
| Required criteria | Insulin resistance | Hyperinsulinemia | None | Central obesity |
| MS present when | + 2/5 criteria | + 2/4 criteria | 3/5 criteria | + 2/4 criteria |
| Obesity | Waist/hip1 or BMI2 | Waist3 | Waist4 | Waist3 (European) |
| Hyperglycemia | Insulin resistance5 | Hyperinsulinemia6 | > 100 mg/dl | > 100 mg/dl |
| Dyslipidemia | TG7 or HDL-C8 | TG9 or HDL-C10 | TG7 and HDL11 | TG7 and HDL11 |
| Hypertension | > 140/90 mmHg | > 140/90 mmHg | > 130/85 mmHg | > 130/85 mmHg |
| Other criteria | Microalbuminuria12 | None | None | None |
1 > 90 cm (M) or > 85 cm (F)
2 Body mass index > 30 kg/m2
3 > 94 cm (M) or > 80 cm (F)
4 > 40 inches (M) or > 35 inches (F)
5 Impaired fasting glucose, glucose intolerance, type 2 diabetes or any other evidence
6 Plasma insulin > 75th percentile
7 Plasma triglyceride > 150 mg/dl
8 High density lipoprotein < 35 mg/dl (M) or < 39 mg/dl (F)
9 Plasma triglyceride > 177 mg/dl
10 High density lipoprotein < 39 mg/dl
11 High density lipoprotein < 40 mg/dl (M) or < 50 mg/dl (F)
12 Urinary albumin excretion > 20 mcg/min or albumin-to-creatinin ratio > 30 mg/g
The MS is clinically important for several reasons:
a) it allows to identify patients with a high risk of developing atherothrombotic complications, DM2, or both;
b) it expands our knowledge on the mechanisms linking their components and the development of atherosclerosis;
c) it has prompted epidemiological and clinical investigation on preventive approaches based on lifestyle and drug therapy
Measuring insulin resistance
Insulin is produced by the pancreas in response to hyperglycemia and stimulates glucose use differently in various tissues (table 2)1.
Table 2. A summary of the effects of insulin in different tissues
| Tissue | Effects of insulin |
| Skeletal muscle | Stimulates glucose uptake (by translocation of the GLUT4 glucose transporter to the cell surface) Stimulates the synthesis of glycogen from glucose Inhibits glycogenolysis |
| Adipose tissue | Stimulates glucose uptake (by translocation of the GLUT4 glucose transporter to the cell surface) Inhibits lipolysis Stimulates glucose uptake |
| Liver | Stimulates the synthesis of glycogen from glucose Inhibits glycogenolysis Decreases hepatic gluconeogenesis |
Insulin resistance (IR) occurs when there is a decrease in the responsiveness of adipose, muscle and liver cells to the action of insulin. As a consequence, circulating insulin and glucose levels remain high, which leads to several pathologic changes. Insulin resistance is linked to several known cardiovascular risk factors (dyslipidemia, hypertension, DM2, obesity) and is a hallmark of many cardiovascular diseases. Therefore, quantifying insulin sensitivity/resistance in humans and animal models has gained more and more importance for epidemiological studies and clinical and basic science investigations, but its use in clinical practice has been scarce.
Direct and indirect methods are currently employed to assess insulin resistance. Established direct methods for measuring insulin sensitivity in vivo are relatively complex. The hyperinsulinemic-euglycemic glucose clamp and the insulin suppression test directly assess insulin-mediated glucose utilization under steady-state conditions, rather difficult to achieve and control; they may be useful for intensive physiological studies on small numbers of subjects. A slightly less complex indirect method relies on minimal model analysis of a frequently sampled intravenous glucose tolerance test. Some surrogate indexes are well-established methods to indirectly assess insulin sensitivity/resistance (e.g., QUICKI, HOMA), that are derived from blood insulin and glucose concentrations under fasting conditions (steady state) or after an oral glucose load (dynamic); these indexes could be more appropriate for large epidemiological studies. The determination of fasting intact proinsulin or the proinsulin/insulin ratio are currently used mostly to analyze the effects of new drugs on the insulin secreting cells3,4.
The ratio of triglyceride to high-density lipoprotein as surrogate marker for insulin resistance
Some surrogate indexes have attempted to help in the recognition of insulin resistance in patients with overweight or glucose abnormalities. In the clinical scenario, the presence or absence of insulin resistance adds nothing to the preventive measures required for a patient with metabolic syndrome; consequently, there are no indications for assessing insulin sensitivity by any of the available methods.
The Spanish MESYAS (Metabolic Syndrome in Active Subjects) group has studied the correlation between TG/HDL ratio and the presence of MS in 18,778 active workers (77.6% men; mean age 42.2 ± 10.7 years) enrolled in 3 insurance companies in Spain from their annual health examinations. Prevalences of MS were 18.8% in men and 6.1% in women. Mean value of the TG/HDL ratio was 2.50 ± 2.2 and increased in parallel to the number of MS components present. Subjects with MS had a ratio that was 2 times higher compared with those without (5.10 vs 2.03, p <0.001). Receiver operating characteristic curves showed that values >2.75 in men and >1.65 in women of the TG/HDL ratio were highly predictive to the diagnosis of MS with 80% sensitivity and 78% specificity5.
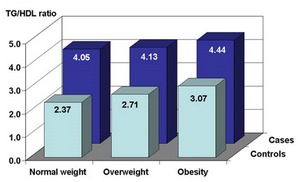
Another more recent study of this group has aimed to correlate the TG/HDL ratio with the incidence of a first coronary event (myocardial infarction, unstable angina or subclinical myocardial ischemia detected through electrocardiogram abnormalities) in male workers according to body mass index (BMI) in a case-control study design (208 cases and 2080 controls, mean age 49.9 years). TG/HDL ratio was significantly higher in cases compared to controls, and a significant increasing prevalence of cases and mean TG/HDL in each category of BMI was present (figure 1). Multivariable analysis demonstrated that TG/HDL increased by 50% the risk of a first coronary event (OR: 1.47; 95% CI 1.26-1.71), meanwhile LDL-C values obtained more moderate increased-risk (OR: 1.01; 95% CI 1.005-1.012); metabolic syndrome (OR: 1.76; 95% CI 0.94-3.30) and hypertension (OR: 1.50; 95% CI 0.81-2.79) did not reach statistical significance. TG/HDL ratio was associated to first coronary event in all categories of BMI6.
A number of studies have shown that the ratio TG/HDL has a good correlation with the generally accepted methods to define insulin sensitivity, with the possible exception of African Americans7. Some drugs (thiazolidindiones, angiotensin and aldosterone antagonists, moxonidine) have demonstrated favourable effects on IR, although we do not have enough data to confirm if TG/HDL also changes in the good direction.
Fig 1 :TG/HDL ratio correlated with the incidence of coronary event in the MESYAS study