1) CRT increases survival for patients with heart failure, but it doesn’t work well in all patients
Heart failure remains a major cause of death and disability, despite the proven morbidity and mortality benefits of pharmacological therapy. Cardiac Resynchronisation Therapy (CRT) has been proposed as a non-pharmacological alternative therapy in these patients. From the early evidence of clinical and functional benefit, it now shows it can also increase survival. Nevertheless, not all patients respond positively to CRT and the medical community wants to find the reason for that.
2) Parameters able to identify responders to CRT have been found
The echocardiographic evidence of mechanical asynchrony has recently been shown to be an independent predictor of outcome. Thus, the presence of mechanical asynchrony seems to have prognostic implications.
Echocardiographic evidence of asynchronous contraction could help predict a positive response to CRT. Echocardiography has been advancing with amazing speed and parameters able to identify responders to CRT have been found.
New sophisticated echocardiographic techniques are evolving, in the effort to overcome the limitations present in several conventional parameters. Indeed :
- Pitzalis et al (1) demonstrated that the presence of a SPWMD ≥ 130 msec, prior to CRT implantation, was able to identify those candidates who showed a significant reduction of HF progression.
- Bader et al (2) demonstrated that the presence of intra-ventricular, but not inter-ventricular asynchrony, assessed by TDI, was an independent predictor of hospitalisation for cardiac decompensation.
- In a study by Bax et al (3), pre-implantation echocardiographic evidence of LV dyssynchrony, defined as the maximum delay between peak TDI velocities among the anterior, inferior, septal and lateral LV basal walls, was associated with a significant better prognosis in the first year after CRT.
- In the CARE-HF study (4), there was a trend for a greater benefit of CRT therapy in patients with a higher degree of interventricular asynchrony.
The QRS width is, currently, the approved selection criterion for implantation of CRT devices (5,6).
However, about 30 % of patients do not respond to CRT and show no evidence of reverse remodelling (7). On the other hand, the presence of mechanical asynchrony was documented in patients with narrow QRS, and this subgroup of patients was also shown to derive a favourable effect to CRT (8-10). Thus, it seems that mechanical asynchrony can be present without substantially increasing the QRS duration on the surface ECG.
3) Curently, the main methods used to detect the presence of mechanical cardiac asynchrony are (11):
M-mode Echocardiography: The septal-to-posterior wall motion delay (SPWMD) was proposed by Pitzalis as a parameter of intraventricular dyssynchrony. It is determined as the shortest interval between the maximal posterior displacement of the septum and the maximal displacement of the left posterior wall in an M-mode tracing from the paraesternal short-axis view at the level of the papillary muscle (Figure 1).
Doppler Echocardiography: Pulsed Doppler flow measurements have been used to identify interventricular asynchrony. Left and right ventricle pre-ejection intervals are measured as the time from the onset of the QRS complex on the surface ECG and the onset of the left and right ventricle Pulsed Doppler waves. Interventricular asynchrony is evaluated by determining the extent of interventricular mechanical delay (IVMD), measured as the time difference between left and right ventricular pre-ejection intervals. An IVMD of more than 40 ms is considered indicative of interventricular asynchrony (4) but its ability to predict response to CRT remain to be proven.
Tissue Doppler Imaging (TDI): The septal-to-lateral delay (SLD), a TDI index proposed by Bax, is measured as the time difference from the onset of the QRS complex and peak systolic TDI wave between the basal septal and lateral walls (figures 2A and 2B), and has proven to be able to identify responders. Furthermore, the value of the TDI derived systolic asynchrony index (TS-SD) has been investigated, in several studies by Yu. This index, calculated as the standard deviation of the time to peak myocardial systolic contraction of 12 LV segments in a 6-basal-6-mid segmental model, was the only independent predictor of LV reverse remodelling after CRT. A pre-implantation TS-SD of 32.6 ms was able to totally separate non-responders from responders.
Strain, strain rate and tissue tracking: In a comparison between TDI and strain rate imaging by Yu, the former showed to be superior on the prediction of reverse remodelling. Tissue tracking was used by Sogaard to demonstrate that the extent of the left ventricular base circumference displaying delayed longitudinal contraction, before pace-maker implantation, was able to predict long-term efficacy of CRT.
Three-dimensional Echocardiography: in a study by Kapetanakis, a Systolic Asynchrony Index (DI) was derived from 3D regional volumetric curves (Figure 3). The DI was defined as the standard deviation of these timings. Higher values denote increasing intraventricular dyssynchrony.
The content of this article reflects the personal opinion of the author/s and is not necessarily the official position of the European Society of Cardiology.
Conclusion:
To conclude, extensive investigation in this field has resulted in several echocardiographic parameters that have been proposed to define asynchrony. The wide diversity of parameters, the variety of aspects of the synchronicity of contraction evaluated in the different parameters, the different definitions of response used in the several studies, and the small number of patients included, can somehow explain the current inability to find a gold standard parameter to be used in clinical practice.
In fact, one of the most interesting findings of the RAVE study (12) was the poor agreement among the different methods to detect asynchrony. The recently shown results of the PROSPECT study, did not confer a great superiority to the echo techniques over surface EKG in the detection of responders to CRT. Future large randomised clinical trials are needed to evaluate these proposed parameters and find an accurate and standardised echocardiographic evaluation criteria of asynchrony.
Figure 1: Septal-to-posterior wall motion delay or Pitzalis method. See text for details.
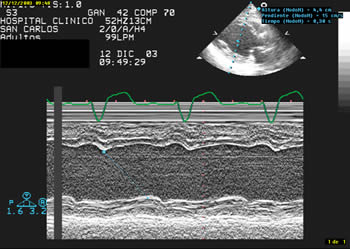
Figure 2A and 2B: Measurement of the septal-to-lateral delay using TDI.
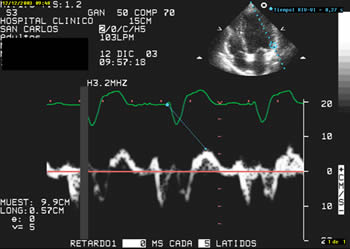
Figure 2B
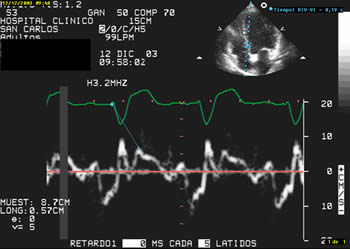
Figure 3: 3D-echocardiography-derived regional volumetric curves.