
Introduction
It is amply recognised that blood pressure (BP) control does not achieve the goals recommended by Guidelines (1,2).
For a goal inferior to 140/90 mmHg :
- In clinical practice
a percentage of control above 30% is rarely seen (3). - in hospital based hypertension units
values above 40% have been described (4) - in some clinical trials such as ALLHAT
the percentage has been as high as 60% (5).
In the last two cases, when, according to Guidelines, a goal below 130/80 mm Hg had been considered - e.g. when associated clinical conditions, diabetes and Chronic Kidney Disease (CKD), are present- adequate BP control is less than 20% in hypertension units (4) as probably the case in most clinical trials.
Attaining adequate BP goal is very difficult, particularly when it comes to systolic BP. What guidelines consider as adequate BP control could be a non-realistic target in daily clinical practice (6).
1) Earlier intervention with drugs.
Both the level of BP and its consequences rise continuously if arterial hypertension is not adequately treated. Progression from prehypertension to established hypertension is a well known fact (7).
If hypertension is not controlled, it progresses with time to more advanced stages and causes the well known increase in cardiovascular (CV) damage and renal damage (8).
Defining the most adequate threshold BP to start pharmacological intervention would impede the evolution of arterial hypertension and thus avoid the progression of CV disease.
- A direct pharmacological intervention, accompanied by lifestyle changes, is contemplated if BP levels are above the limit defining stage 2 in arterial hypertension (> 160/100 mmHg).
- In the remaining cases, threshold BP is defined as the persistence of BP values above 140/90 mmHg after a period of adequately performed life-style changes.
- Furthermore, both JNC-7 and ESH-ESC Guidelines (1,2) recognise the existence of compelling indications that admit starting treatment even when BP levels are in the range of prehypertension. This is the case when target organ damage (TOD) or associated clinical conditions (ACC) are present.
In daily clinical practice intervention frequently takes place when BP levels are clearly above the levels recommended by Guidelines. Furthermore, once pharmacological therapy is started, clinical inertia (9) greatly contributes to facilitate the absence of a good BP control due to the acceptance by doctors of elevated BP levels as adequate for the patient.
The possibility of preventing the development of arterial hypertension through adequate lifestyle, in particular if obesity is corrected, has been demonstrated (10).
Pharmacological intervention directed at preventing the development of arterial hypertension (BP > 140/90 mmHg) has been recently suggested (11). The TROPHY study tested the hypothesis that pharmacologic treatment of prehypertension prevents or postpones stage 1 hypertension.
The study contemplated a follow-up of four years;
- during the first two years, candesartan, an angiotensin receptor blocker, was compared to placebo.
- in the last two years all the patients received placebo.
Active therapy decreased the risk of developing stage 1 hypertension by 66.3% (p < 0.001) during the first two years. At the end of the study the risk was still reduced by 15.6% (p < 0.007) in those patients who had received the active medication.
The transition from prehypertension to established hypertension reflects, in part, ongoing changes such as arteriolar hypertrophy (12) and endothelial dysfunction (13). In this sense, prehypertension is characterised by the existence of elevations in plasma norepinephrine and plasma renin concentrations (14,15) that could promote growth and endothelial dysfunction. Regression of arteriolar hypertrophy has been shown to occur when treatment with an angiotensin converting enzyme inhibitor (ACEI) or an angiotensin receptor blocker (ARB) are given (16,17). This does not occur in the presence of a beta blocker.
These data stress the consideration that an earlier intervention with drugs in daily clinical practice could facilitate the attainment of a much better BP control facilitated by the regression of the vascular changes accompanying the increase in BP from the initial stages of the process.
Furthermore, it has been demonstrated that BP, within the range of prehypertension, is associated with an elevated risk of cardiovascular disease (18,19) beyond that attributable to accompanying situations such as diabetes, TOD or established CV disease and partly attributable to the association of prehypertension with other CV risk factors (20,21). Early pharmacological intervention in arterial hypertension must then be contemplated in order to diminish the early development of CV disease.
2) Combination therapy from the onset of treatment.
An apparent discrepancy in the choice of the first drug exists between JNC-7 (1) and ESH-ESC (2) guidelines.
- JNC-7 defends the use of diuretics in most patients as a first step therapy to get a significant decrease in the high risk that accompanies elevated BP and thus achieving it at the lowest cost.
- On the contrary, the ESH-ESC guideline defends the need for individual therapy in each patient admitting that any drug available can be considered as adequate for first step therapy.
The demonstration that arterial hypertension is the number one risk factor in promoting death in developed as well as in developing countries (22) fits well with the concept of JNC-7.
However, the fact that, prehypertension today, correlates particularly well with insulin resistance (23) forces the consideration that the benefit of simply lowering BP could not suffice to correct the medium-term risk of elevated BP. In fact, the idea of targeting prediabetes in hypertensive patients has been recently brought forward (24) because it is a situation frequently seen in clinical practice, the one where the choice of the antihypertensive drug is relevant to promote, prevent or delay the development of diabetes.
It is also true that the discussion regarding which monotherapy is most adequate seems inapropriate if we consider the elevated percentage of patients requiring combination therapy to obtain adequate BP control. Only 22-24% of people in clinical trials actually achieve blood pressure goals with monotherapy. In fact, unwanted metabolic effects of certain antihypertensive drugs are attenuated when used in combination with members of other classes of antihypertensive agents particularly, with drugs that suppress the renin-angiotensin system (25). The possibility of using a combination, either free or fixed, since the beginning of pharmacological therapy in hypertensive patients is contemplated in both guidelines (1,2). Implementing this possibility probably will contribute to improve BP control due to the higher capacity of the combination to lower BP.
3) Therapy adjusted according to age.
Recently a new version of the British Society of Hypertension Guideline (26) has been published. The recommended choice of the first antihypertensive drug is based on the fact that hypertensives can be broadly classified as “high renin” and “low renin”. Drugs can be divided according to their effects on the renin-angiotensin system (RAS) into those:
- with a capacity to inhibit ACE inhibitors/angiotensin receptor blockers (A) or beta-blockers (B)
- and those without effects on the system, calcium antagonists (C) and diuretics (D).
As can be seen in figure 1, patients under the age of 55, with the highest activity of the RAS, deserve, as first drug, one included in group A or B, while those above the age of 55 would receive one of group C or D. The need for a combination should be covered by adding a drug from the other group (C or D for A or B and vice versa).
If three drugs are required A+ C+ D should be the ideal combination.
This algorithm of treatment is based on the previous experience of the authors which indicates that BP control is more adequate following the recommendation of the British Guideline (27).
For comparison, an algorithm put forth for patients with kidney disease and /or diabetes that integrates both the JNC 7 and ESC/ESH guidelines is noted in figure 2. In contrast to the British guidelines which focus on the general hypertensive patient, this algorithm focuses on the most prevalent concomitant diseases in the older hypertensive patient with a focus on achieving goal blood pressure (28).
4) An aggressive attitude in patients with Associated Clinical Conditions or advanced target organ damage.
Several factors have been identified as potential impediments for the attainment of adequate BP control. They are generally related to an inadequate lifestyle in particular diet containing an excessive amount of salt, an excessive number of calories facilitating an increase in body weight, an excess in alcohol intake, or a low intake of fruit and vegetables, Table 1.
Other factors are related to inadequate doses of antihypertensive drugs, inadequate combinations or to accompanying therapies interfering with antihypertensive therapy.
However, there is an important predictor of the need for multiple antihypertensive therapy, the degree of CV and renal involvement as a consequence of the increase in BP. The presence of Associated clinical conditions or advanced target organ damage renders control of BP more difficult and the need for more medication to acheive it (29). An aggressive attitude is required for the treatment of these patients because the adequate level of control is inferior to 130/80 mmHg.
5) Favouring long-term adherence to treatment in patients.
Many patients do not take their prescribed medications. In most surveys one fourth to one half of patients had abandoned their antihypertensive drugs one year after starting therapy (30). It is also true that many physicians do not prescribe all the required medications required to control BP in their patients (9). The reasons for a low compliance and for such poor long-term adherence are diverse but in particular poor tolerability has been claimed as one of the most important. Table 2 summarises Guidelines directed to improve maintenance of antihypertensive therapy according to Norman Kaplan (31).
6) Public health authorities to set up an economic system that reinforces health behaviour.
Cardiovascular and renal disease have been described as a continuum (32) starting with the detection of CV and renal risk factors, followed by the detection of target organ damage (TOD) and finally by ACC and eventually death. It is clear that lifestyle interventions can clearly delay the development of hypertension as well as reduce CV risk, Table 1.
It is inadequate for only physicians and health care professionals to discuss such issues. Public health authorities need to intervene and set up an economic system that reinforces health behaviour. As a paradigm this has occurred in Finland with a dramatic reduction in the CV events within the last decade.
Table 1
Lifestyle Modifications and Effects on Blood Pressure
From Chobanian A et.al. (1).
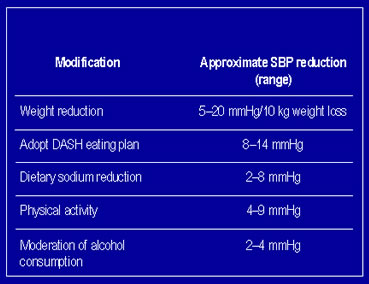
Table 2
| Guidelines to improve maintenance of antihypertensive therapy. Summarised from (30) |
|---|
| - Be aware of the problem and be alert of signs of inadequate intake of medications |
| - Articulate the goal of therapy with few or no side effects |
| - Educate the patient |
| - Maintain contact with the patient |
| - Keep care inexpensive and simple |
| - Prescribe according to pharmacologic principles |
| - Be willing to stop and substitute unsuccessful therapy |
| - Anticipate and address side effects |
| - Continue to add effective and tolerated drugs |
| - Provide feed-back and validation of success |
Figure 1
Recommendations for combining blood pressure lowering
drugs (AB/CD rule) (From reference 26, Williams et al)
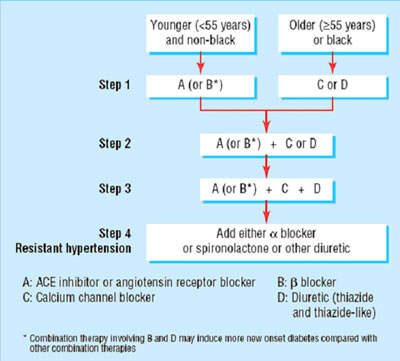
Figure 2
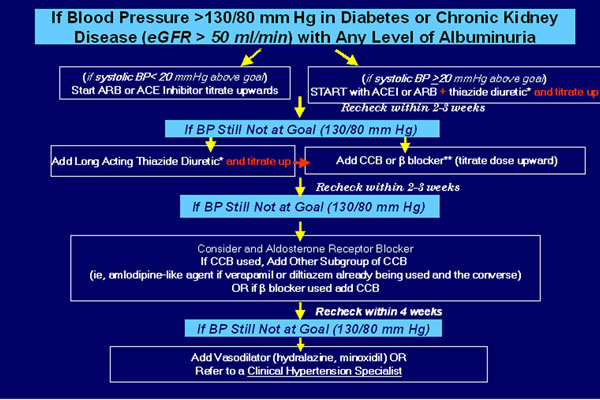
Legend
Exercise caution over the use of high doses of diuretics.
If a beta blocker is prescribed then it should be combined with a DHP CCB.
** Carvedilol has been shown to be beneficial in renal impairment and outcome studies. Other beta blockers are not excluded, however, there are no renal outcome data to support the use of atenolol in such patients and only limited data to support metoprolol (AASK trial, Toprol XL). Additionally, other alpha/beta blockers such as labetolol, may be useful but have not been studied in this population.
eGFR = estimated glomerular filtration rate (most currently accepted method for Stages 2 through 4-modified MDRD formula(GFR calculator can be found-www.kidney.org; http://www.nephron.com/ and multiple other websites); BP = blood pressure; ARB = angiotensin II receptor blocker; ACEI = angiotensin-converting-enzyme inhibitor; CCB = calcium channel blocker; DHP CCB = dihydropyridine calcium channel blocker; RAAS = renin-angiotensin-aldosterone system.
The content of this article reflects the personal opinion of the author/s and is not necessarily the official position of the European Society of Cardiology.