
The epidemiological studies have indicated that hypertension and type 2 diabetes are commonly associated conditions and their concordance is increased in populations. Hypertension affects up to 40% or more of diabetic patients (1, 5, 6). However, the independent effect of type 2 diabetes or hyperglycemia on stroke risk has been found inconsistent; some (7-14), but not all studies (15-17) have identified type 2 diabetes or hyperglycemia as an independent risk factor for stroke. Although there are few studies (12, 14) concerning the joint prognostic effect of hypertension and type 2 diabetes on stroke risk in the general population, it is not well known whether the increasing risk of stroke comes from the effect of hypertension or type 2 diabetes alone, or from the combined effect of both hypertension and type 2 diabetes.
An evaluation of the joint association of history of hypertension and type 2 diabetes on the incidence of stroke and stroke mortality
We evaluated prospectively the joint association of history of hypertension and type 2 diabetes on the incidence of stroke and stroke mortality among 49,582 Finnish participants, who were aged between 25 and 74 years and who were free of stroke and coronary heart disease at baseline (18). During a mean follow-up of 19.1 years, 2978 incident stroke events were recorded, of which 924 were fatal. The association between hypertension and increased risk of stroke incidence and stroke-related mortality was consistent among diabetic and nondiabetic patients.
After adjustments for age, sex, body mass index, cholesterol, education, smoking, alcohol consumption, and physical activity, increased hazard ratios (HR) for incident stroke of 1.33 and 1.90 were observed for patients with hypertension stage I (blood pressure 140-159/90-94 mmHg and without any antihypertensive drugs treatment at baseline) and stage II (blood pressure ?160/95 mmHg, or using antihypertensive drugs at baseline) (Figure 1). Patients with diabetes had an increased HR of 2.50 compared with those who did not have the condition. In patients with both diabetes and hypertension stage I, the HR was raised to 3.30 and in those with diabetes and hypertension stage II it was increased to 4.09.
Increased HRs of 1.47 and 2.51 for stroke mortality was found for patients with hypertension stage I and stage II, respectively, compared with those who had normal blood pressure (Figure 2). Diabetes alone gave a HR of 2.94, diabetes with hypertension stage I raised the HR to 5.22, and the combination of diabetes and hypertension stage II increased the risk of death from stroke by more than eight times, with an HR of 8.01.
A large proportion of stroke cases thought to be related to hypertension might also be attributable to unrecognized type 2 diabetes
The result from our study shows that hypertension and type 2 diabetes are independently linked to increased risk of stroke incidence and stroke-related mortality; these risks are greatly increased in patients with both conditions. Because hypertension and type 2 diabetes often occur concomitantly, it is possible that a large proportion of stroke cases thought to be related to hypertension might also be attributable to unrecognized type 2 diabetes.
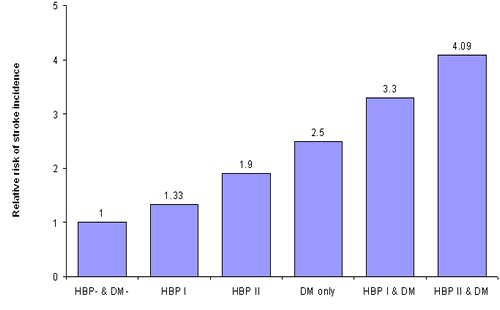
Figure 1. Hazard ratios for stroke incidence according to the history of hypertension and diabetes at baseline. Hypertension I was defined as blood pressure 140-159/90-94 mmHg and without any antihypertensive drugs treatment at baseline; hypertension II was defined as blood pressure ?160/95 mmHg, or using antihypertensive drugs at baseline; the normotensive reference group was defined as blood pressure <140/90 mmHg and without any antihypertensive drugs treatment at baseline; adjusted for age, sex, study year, BMI, cholesterol, education, smoking, alcohol drinking, and physical activity.
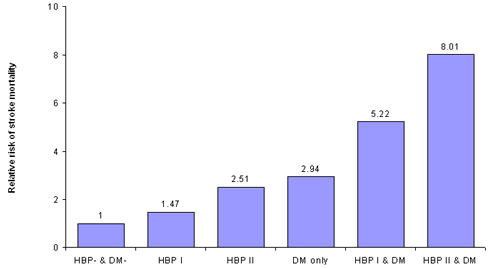
Figure 2. Hazard ratios for stroke mortality according to the history of hypertension and diabetes at baseline. Hypertension I was defined as blood pressure 140-159/90-94 mmHg and without any antihypertensive drugs treatment at baseline; hypertension II was defined as blood pressure ?160/95 mmHg, or using antihypertensive drugs at baseline; the normotensive reference group was defined as blood pressure <140/90 mmHg and without any antihypertensive drugs treatment at baseline; adjusted for age, sex, study year, BMI, cholesterol, education, smoking, alcohol drinking, and physical activity.
The content of this article reflects the personal opinion of the author/s and is not necessarily the official position of the European Society of Cardiology.